
Conjugated Rehab
Guest Author: Jeremy Aspa (MS, LAT, ATC, USAW, CDNLVL 1)- Athletic Trainer at United States Air Force
Follow Jeremy on Instagram
My closest colleagues in the strength realm understand that I’m very biased towards conjugate periodization. Why? Frankly, I'm honestly still trying to figure out exactly why. A lot of strength professionals I’ve come into contact with are either with it or against it. But in all seriousness, I’m just a fan of this approach, and I can’t ignore the results I’ve had with my athletes. The methodology speaks to me. Not to mention I’m a huge enthusiast of the Westside principals and mentality. The operative component to the conjugate system is that it can be manipulated however you want based off the needs of the athlete; and this is the case whether we’re talking elite level powerlifters, or rehab and restorative strength for athletes and general population.
A couple years ago I thought, if the conjugate system works in the powerlifting and athletic populations, why wouldn’t it work in an orthopedic rehabilitation setting? More specifically, in a traditional athletic training setting such as a Division-I athletic setting. I’m fortunate to have a high volume of contact with my athletes, granting me a lot of time to rotate different systems. If you break down the conjugate system, it focuses on weaknesses, optimizes recovery, and ultimately promotes health and longevity in the organism, while at the same time allowing them to always be ready to perform at a high level. Isn’t that what we would want in a rehab program? Obviously, it is not a wise approach for immediate post- surgical cases, but what about the cases that aren’t post-surgical? In my work setting, it’s extremely common for athletes to continue to compete with some type of chronic injury, especially in season.
Working in college athletics for a handful of years, I’ve always had athletes that experience moderate amounts of pain although while remaining functional. In many instances, these injuries would begin in the middle of their preseason and sometimes last to nearly the end of the regular season. The chronicity of their pain is way ahead of their body’s ability to heal and repair for most of these athletes. In my first couple years of working in the field as an athletic trainer, I would build up a rehab program that would eventually be so immense in volume that they’d be extremely fatigued from the previous days rehab session. When they came in to see me the following days, they wouldn’t be ready to rehab due to their accumulated stress over time. To my own fault in the past, athletes would be constantly doing high volume isolation work, more functional movement, plyometrics, and slower velocity strength work. What I was missing, however, is not accounting for the body’s demands in weight training, conditioning, and practice. I’ve even witnessed in some cases, despite doing so much rehab, athletes who would still decline in strength and function. With the external pressures of coaching staffs and needing to have roster depth, there needed to be another way to approach treatments and rehab better because it was the athlete’s job to compete.
It was through this recollection of thoughts that I decided to adopt the conjugate system of methods within my own rehabilitation philosophy for the athletes I worked with. In my opinion, I think that in doing so it beautifully bridged the gap between the functional side of rehab and the performance piece for my athletes to safely remain on the field. It maintains the continuity within the athlete’s holistic plan to continue to perform maximally and optimally. This is why I feel that healthcare practitioners working with high performance athletes need to truly understand the perspective of periodization and strength training outside of the “only bodybuilding” and the “three sets of ten repetitions mentality”. In doing so, it made me a better clinician and did more of a favor overall with my athletes under my supervision of care.
This isn’t a complete lecture series on conjugate periodization, but rather why I chose to use it for my athletes for rehab. I could be completely off my rocker here and most rehab practitioners may call it bullshit, but anecdotally I have gotten extremely great results. If you are not familiar with conjugate periodization and/or would like to take a closer look and dissect the training methodologies of conjugate training, I recommend reading Louie Simmons’s Westside Barbell Book of Methods or refer to Elitefts.com and study their dense catalog regarding all things westside and conjugate training.
For those of you who are extremely familiar with the conjugate system, you will notice that my reasoning for using this system in my rehab isn’t any different from why a powerlifter or an Olympic weightlifter would utilize this for their weight and conditioning training. So, with that all being said, here are three reasons why I’ve gravitated to the conjugate rehab with my non-surgical rehab cases.
REASON 1: ADAPTATION/MANIPULATION
What is the conjugate system? There are many definitions; in a nutshell the conjugate training system utilizes 4 main lift days. Those days include 2 days dedicated to the max effort method where maximal loads move at slow velocities. One day being a max effort upper body day, and another being a max effort lower body day. Next are the other 2 days dedicated to the dynamic effort method at which the lifter moves sub maximal weights at higher velocities to train a higher rate of force development. Those 4 intense workouts would be separated roughly 72 hours apart with bodybuilding, conditioning, and functional workouts in between (the other days). The week for example would present as Monday ME Lower, Wednesday ME Upper, Friday DE Lower, Sunday DE Upper.
My thought process in rehab is that once I understand what we are rehabbing in terms of the involved structures, we can thoroughly understand the weaknesses we need to address. Louie Simmons of Westside Barbell always mentions that mathematically, a pyramid is only as tall as its base. By continuing to build a wide strength base, it trains the shoulders to be strong in awkward positions and movements. With weakness identification, we can thoughtfully map out and seek the adaptations we need. In chronic situations where the athlete will have flare ups of pain during a competitive calendar year, we can then manipulate variables and identify new weaknesses while chasing the same positive results. Ultimately, we are not reverting back to the same ways, rather seeking to understand different pain generators.
Utilization of conjugation can allow us to freely manipulate the program week by week in real time based off if the athlete is progressing or regressing. Allowing us to continually change the modes of how we are delivering certain movement patterns and stimuli allows the athlete to continue to master different contractions, velocities, and angles to ensure a confident command of his or her shoulder movement. It allows to train awkward planes in which injury occurred. Again, if it’s a chronic occurrence, having 2- or 3-week waves of a different max effort and dynamic effort intent ensures us that we are continuously challenging the organism without sacrificing our end goal of being functional and pain free.
I follow roughly a 48-hour window between harder rehab sessions to ensure better tissue recovery between sessions. Though we are not lifting, nor is rehab extremely CNS taxing, it allows the athlete to be more compliant of his or her program. It also decreases psychological burnout that comes with rehab by just going through the motions. Not to mention it safely allows us to chase our adaptations we want to elicit in a methodical fashion. Like lifting, it ensures that we are constantly changing and cycling different variations. We can rehab based on needs and allows the athlete to train what they tend to ignore because they dislike it. It’s important to rotate different stimuli on the same patterns to not only get better, but to simply become stronger. If I can compare it to a weightlifting analogy, I would much rather have an athlete strong in multiple squat variations than just have them being good at a straight bar back squat.
REASON 2: OPTIMIZATION
Another reason I love this approach is that we continue to rehab at an optimal rate. Some days are intense, and some days are just volume work to build up weak muscles. Overall, we continue to rehab, but still ride the force velocity curve. This is extremely important to me especially in season. It bothers me when rehab actually becomes a factor contributing to chronic residual pain and tendinopathies develop from overuse because volume is way too high. A study by Magnusson et al, 2010 revealed that there was a net loss of collagen production 24-36 hours post heavy exercise with very heavy loads. This leads me to realize that even in rehab we can’t overlook that tendons need recovery to allow adaptation to occur. This may explain the reasons why athletes in some cases can develop tendinopathy and residual pain after rehab. Doing too much with improper volume dosages paired with inadequate rest maybe pushing the athlete backwards in the healing process.
Occupation and sport will demand different needs, but in a rehab world I’m thinking, how can I bullet proof the area I’m rehabbing? I need to make sure that the body part accepts max force from external forces and make sure the body part can produce and redirect forces in different and awkward planes. The conjugate system is a way to monitor total volume, central nervous system load, recover better from the previous rehab session, and vary the modes of intent. In my work, it provides a great way to optimize rehab over the course of a competitive calendar year.
We don’t need to just be more fit within our joint, but we need to ensure function and coordination through optimal motor outputs. On days that are mostly isolation focused, such as doing classical rehab exercises, it’s a great way to work both general physical preparedness of the joint from an endurance standpoint, as well as prepotentiate muscle groups before a lift or practice.
REASON 3: INTENT OF METHODS
Constant use of only a singular method makes your adaptations stall. We covered earlier that too much too soon is a no go. Let’s visit the max effort method. Using this method of training in a rehab setting doesn’t necessarily mean lifting maximal loads at slow velocities all the time, but rather having a max “EFFORT” intent such as holding an isometric contraction at a certain angle of a range of motion. In this case, the intent was a max effort because the effort was indeed maximal of the athlete in order for them to hold that position. This technique allows us to safely work certain ranges of motion that might be dysfunctional. On the flip side to that, we can properly micro dose and utilize the dynamic effort method such as sub maximal loaded throws to ensure we do not lose the capacity to generate high rates of force production. Whichever method you choose to use, we must always make sure that we are monitoring accumulated volume over time. Remember the goal is to maximize our exercises without running the risk of breaking the athlete down and having negative effects. Having intent of movement always matters.
APPLICATION
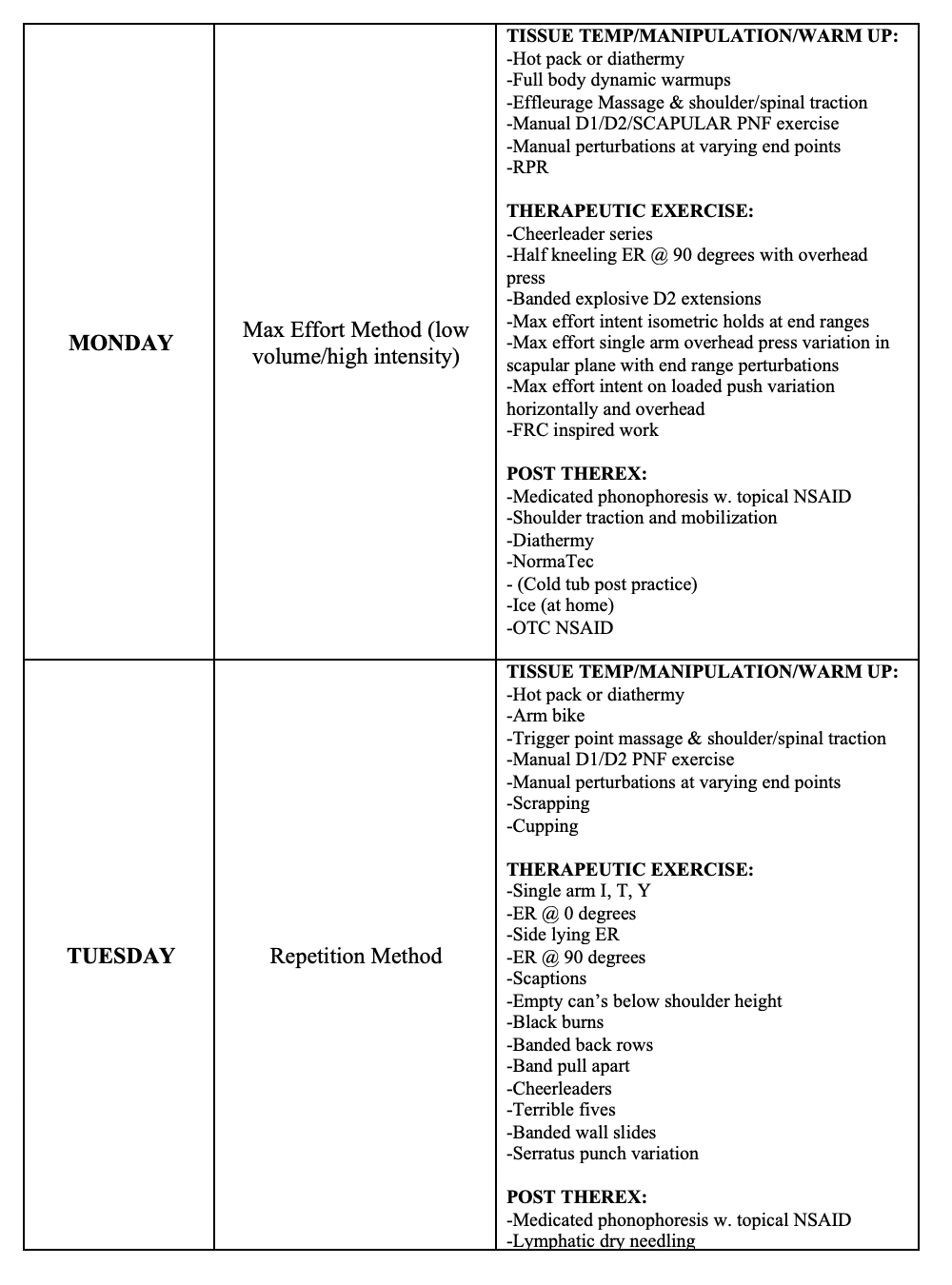
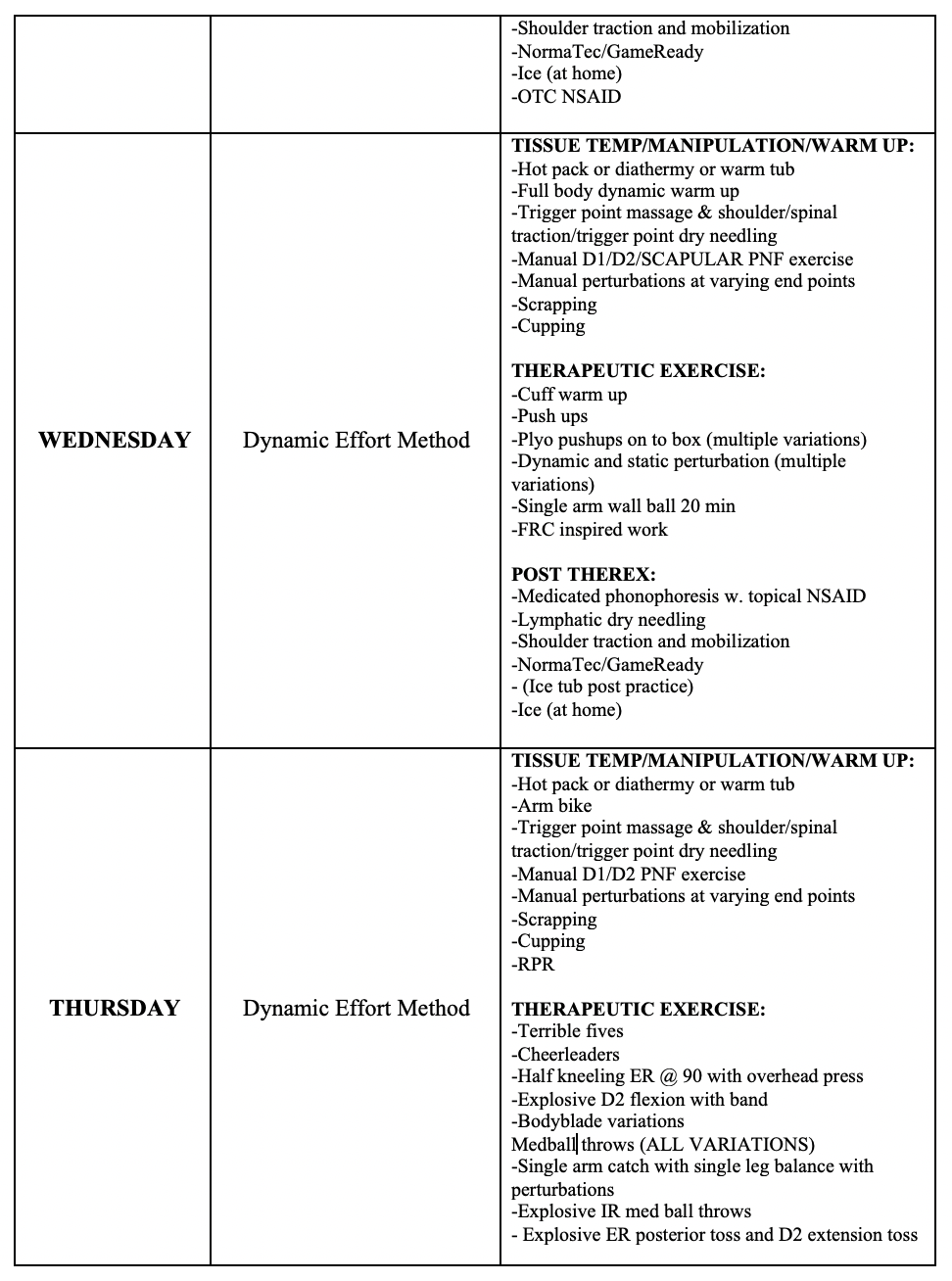
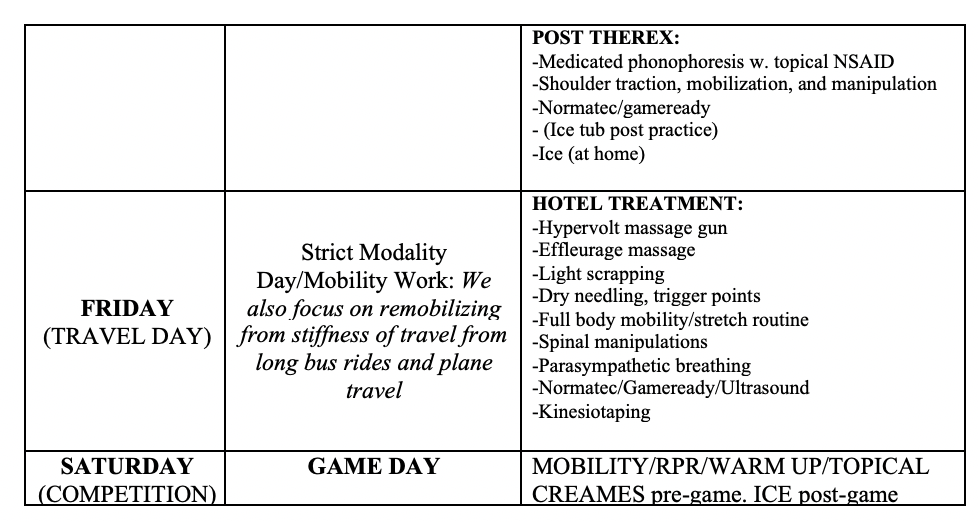
So, what does all this tangibly look like? Below is a snapshot of what a typical week can look like in season for me with Men’s Lacrosse. I will use a slightly similar case I had this season for illustration purposes.
Patient Profile:
Patient: 20-year-old male
History: Chronic right anterior shoulder pain. History of right shoulder arthroscopic labral repair from previous season.
Chief complaint: Experiencing anterior shoulder pain in right shoulder again after completing preseason training camp. No new dislocations or macro traumas.
Diagnosis: General capsular pain/irritation from chronic inflammation
Differential Diagnosis: Rotator cuff strain, bursa irritation
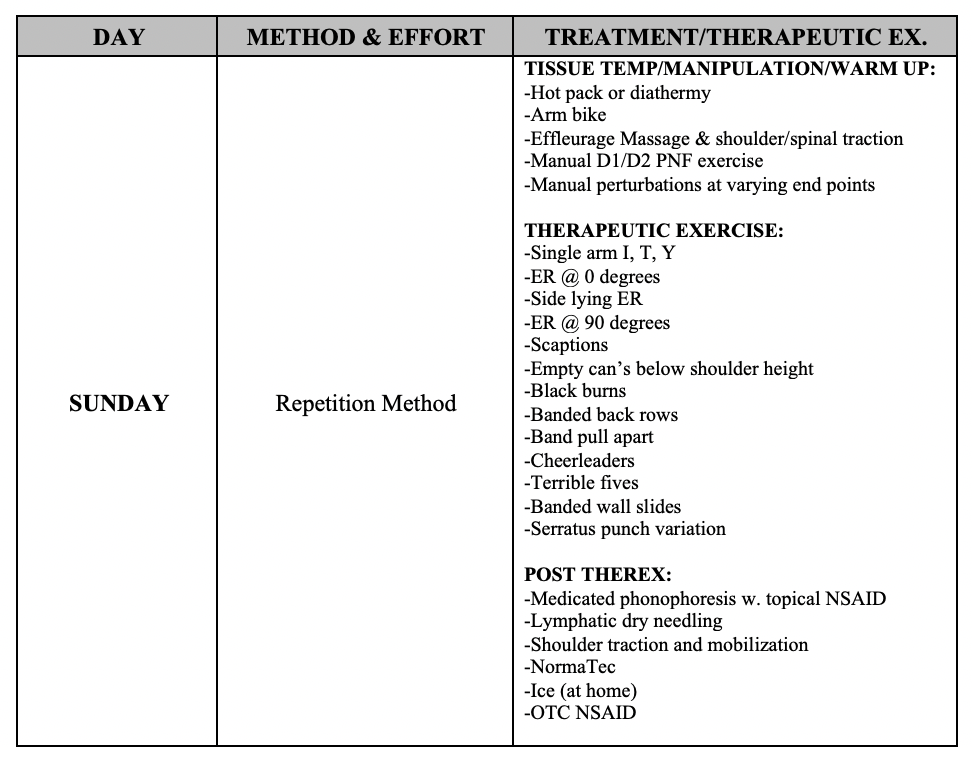
I typically include a separate home exercise program for each of my athletes. It includes only a handful of exercises for extra cuff work that can be done without my assistance just to get another quick session of muscle activation work at home. This is to be done in the evening before bed when we are not traveling. This promotes continued micro dosing rehab sessions over time.
This chart represents a small snapshot out of an entire year. Again, I switch things up frequently in 2-3-week waves. However, I think the proof is in the pudding. For example, an average NCAA Division – 1 men’s lacrosse roster is typically about 44 players. With 10 players on the field at a time, a 44-man roster allows for substitutions if a position player needs some rest. This last season we only had 25 players total, but only 22/23 traveled. We had 3 home games and 10 away games. Before the COVID pandemic cancelled NCAA competition for the rest of the 2020 spring season nationwide, I’ve had almost everyone available for every single game. The only time I had someone not available for a game was due to either a concussion or a massive acute trauma. And with the acute trauma, the athlete only missed 1 game. Overall, everyone was healthy from a soft tissue perspective and everyone was in incredible shape. I whole heartedly believe that this was made possible from the execution of the conjugate piece in the weight room I implemented as their strength coach and the conjugate piece I implemented in the training room as their athletic trainer. The beauty of all of this, is that I had full control of their training and rehabilitation with the conjugate principals as the glue that kept them together. In my opinion, an intelligent healthcare clinician wielding these concepts, can dramatically make your job easier from an injury standpoint. The only way to find out, would be to implement them firsthand.
