
Essential Anatomy for the Foot-Ankle Complex
The foot-ankle complex is one of the most important and paradoxically underappreciated biological structures in the human body. From elite athletes to general population, directly training the foot-ankle complex should be a priority in programming. Beyond its role in sprinting, cutting, and jumping, the foot-ankle complex is essential for posture, balance, and kinetic stability by providing our terminal foundation. I see the foot-ankle complex as effectively being the origin of force interaction, and in many ways has a direct influence on kinetic sequencing and movement expression. In this article, I’d like to cover a thorough breakdown of foot-ankle anatomy and biomechanics, along with discussing how this anatomical junction directly influences and contributes to movement.
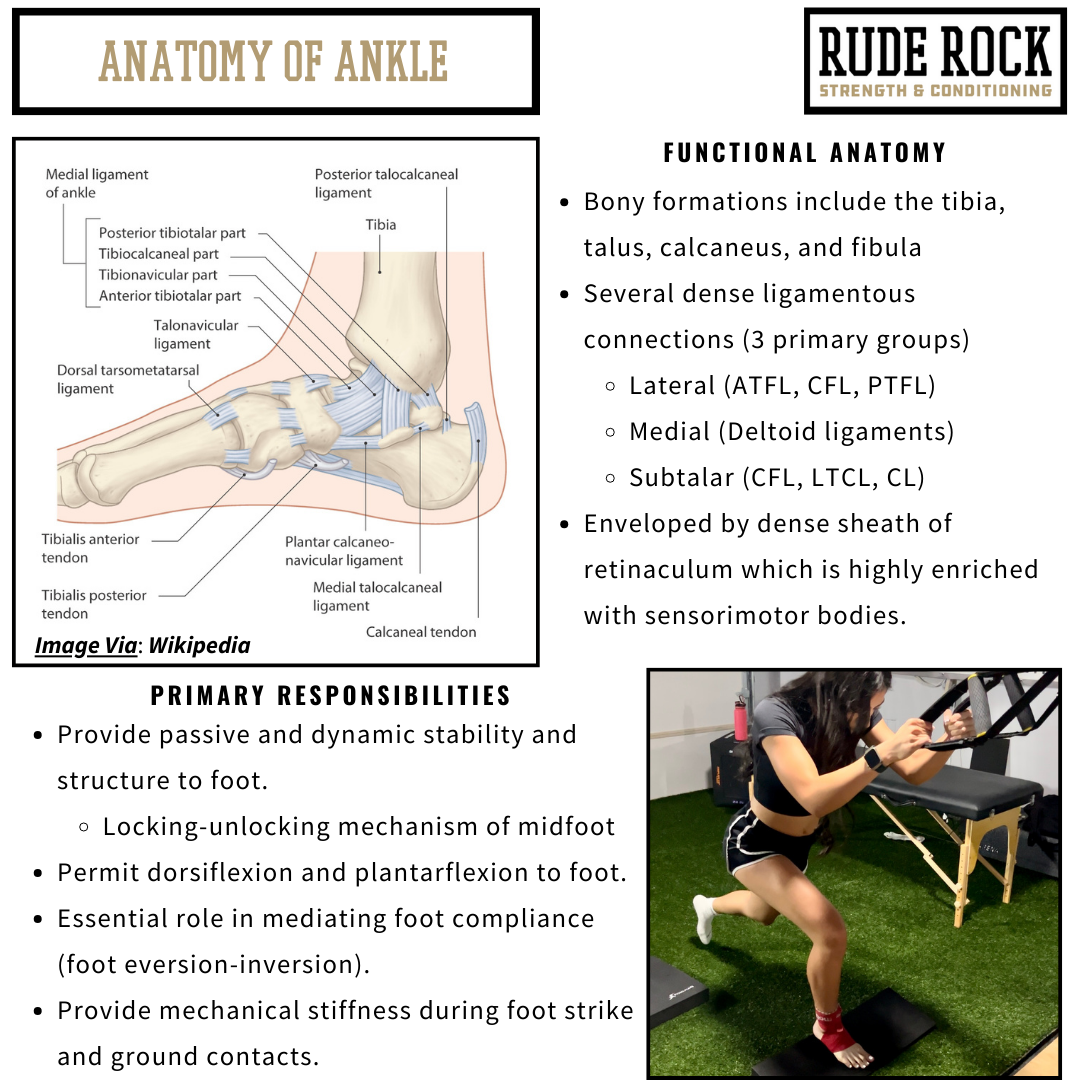
Functional Anatomy of Foot-Ankle Complex
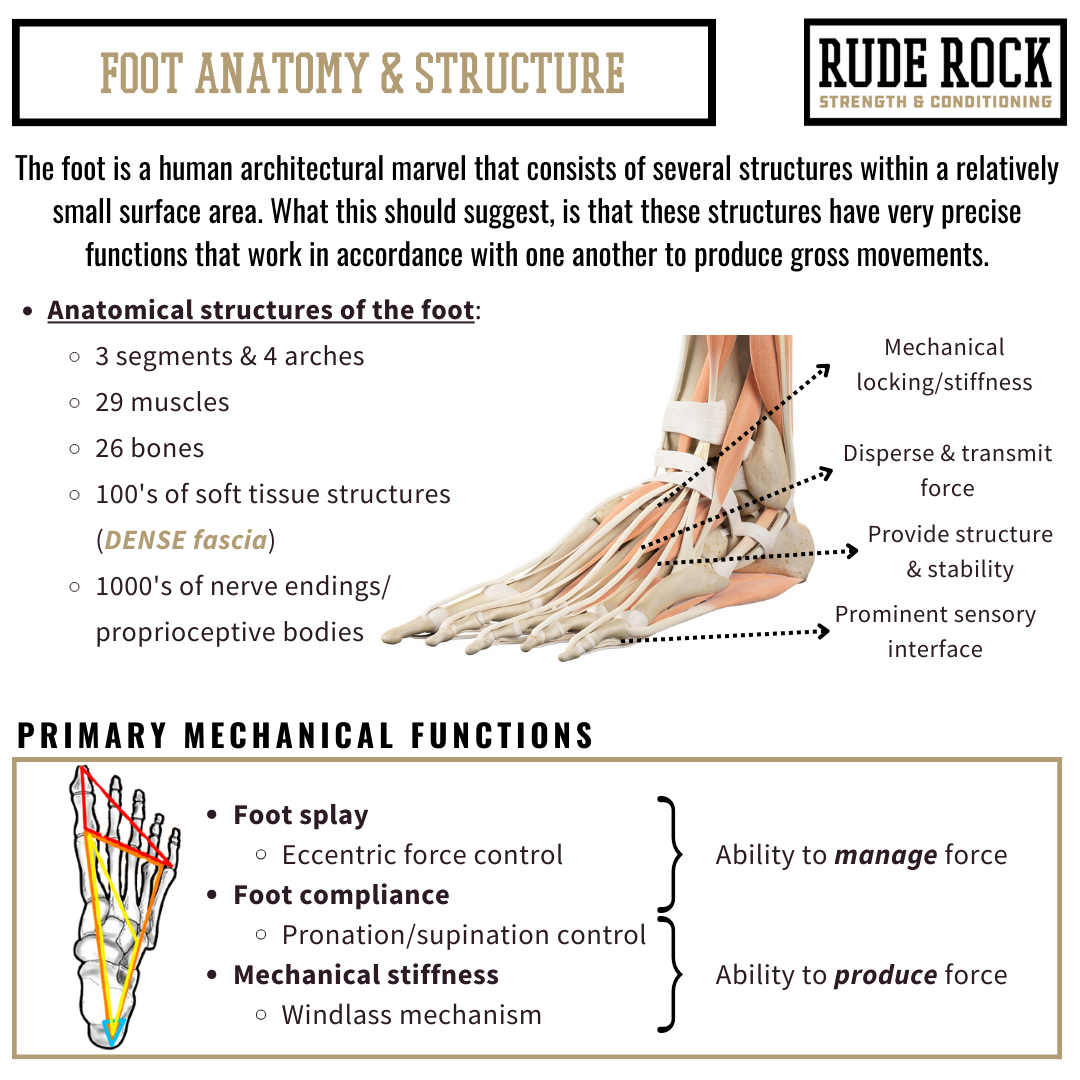
The foot-ankle complex is made of several independent structures and tissues that each provide specific functions to produce collective outcomes. Each foot is made up of approximately 28 bones, 29 muscles, 33 joints, 112 ligaments, several small tendons, and countless (thousands) of free nerve endings and sensorimotor bodies (1). The foot is embedded with several dense connective tissues that collectively form a robust stability network, along with a thick retinaculum enveloping the talus and ankle joint. Considering the relatively small surface area of the foot, it should speak volumes that there are so many tissues and structures confined to such a small space. The way I have always viewed this is that if we consider the number of structures relative to the small surface area, each muscle, joint, bone, and supporting connective tissue must provide an intricate contribution to proper function.
The foot-ankle complex is a perfect illustration of how human anatomy and mechanics are the summation of several structures performing independent functions in tandem to produce global outcomes. With our contemporary pedagogy we have an inclination to see the body as being an assembly of independent parts that are organized and function like robotics. Obviously, this isn’t the reality, as these mechanical relationships are much more symbiotic and entangled than they are isolated from one another. Once again, the foot is a great representation of this. The coordination and integrative function of these structures and tissues is essential for movement mechanics, to include our ability to accommodate and express forces.
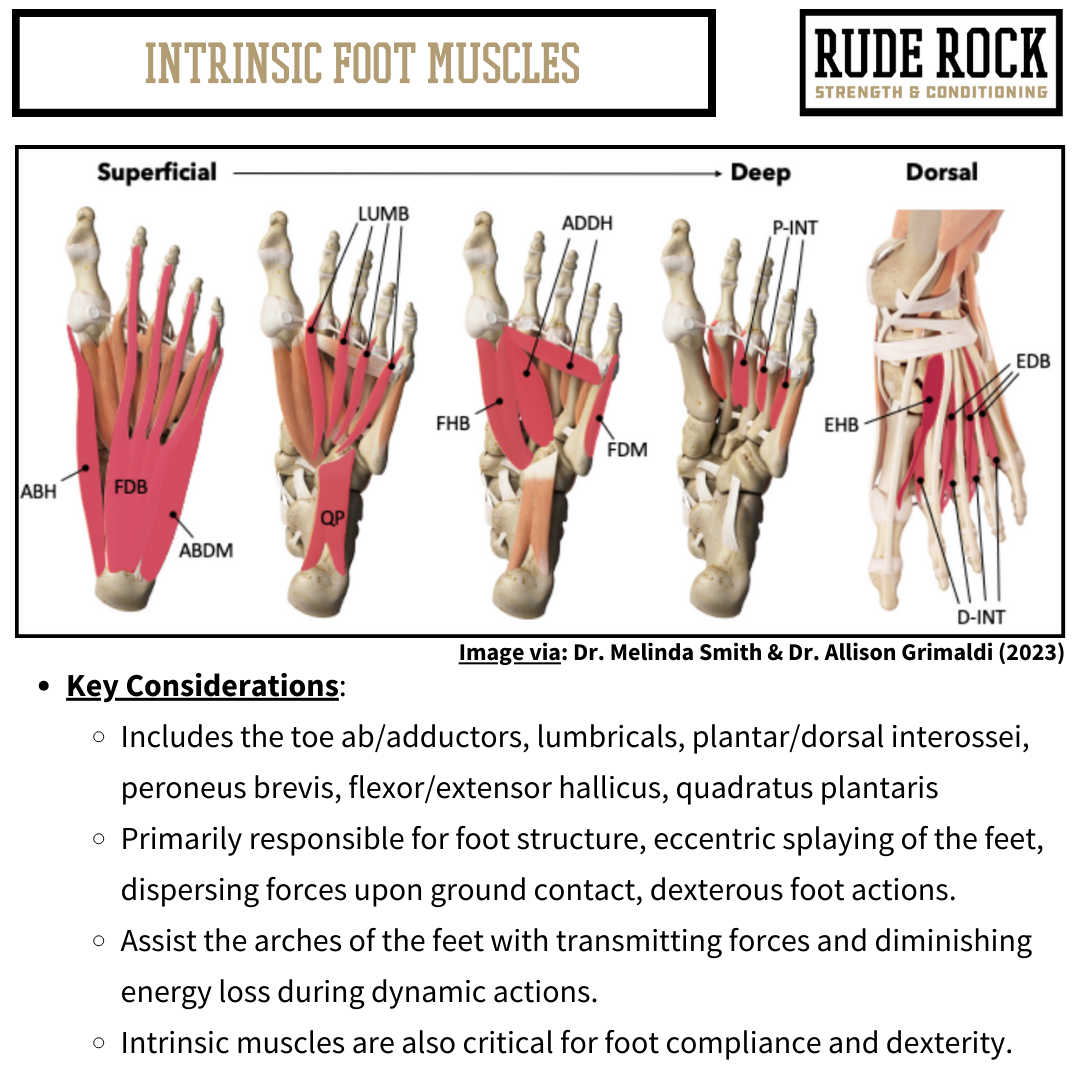
The muscles of the feet can be broadly organized by intrinsic and extrinsic foot muscles. Of the 29 muscles of the foot, 19 are classified as intrinsic muscles account, while the extrinsic account for 10 (2). The intrinsic foot muscles are smaller, deeper muscles that are primarily responsible for providing stability and structure to the foot while also moving (“splaying”) the toes. The extrinsic foot muscles are the bigger, superficial muscles that are primarily responsible for gross motor actions of the foot-ankle complex such as dorsiflexion/plantarflexion. These muscles include the gastrocs, soleus, peroneals, and poster-anterior tibialis muscles. Similarly to how there is an inherent relationship between the three segments of the foot, the intrinsic and extrinsic muscles work in tandem and have an inextricable role in foot mechanics and function.
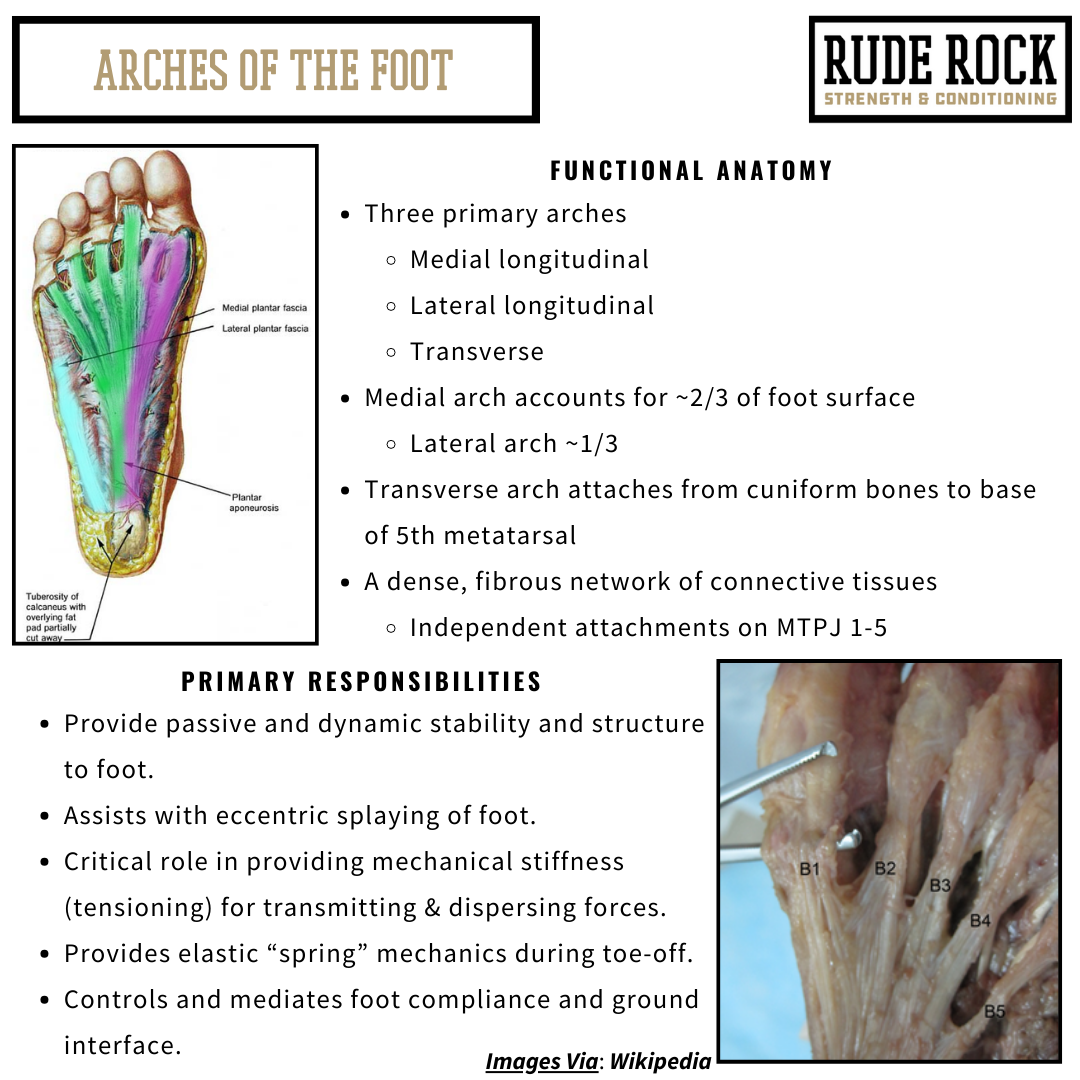
There are 3 (or 4) primary arches of the feet, and the arches play several significant roles for foot function. Primarily the arches are responsible for providing passive and dynamic structure and stability to the foot. The arches work in tandem with the intrinsic foot muscles to help with compliance and stability across various points of the foot, along with the actions of splaying and dispersing eccentric forces upon ground contact. The arches are also notably the primary structure responsible for storing and releasing mechanical energy during toe-off, which occurs predominantly through the medial longitudinal arch. This function is what allows our gait to be “springy” and propulsive during toe-off.
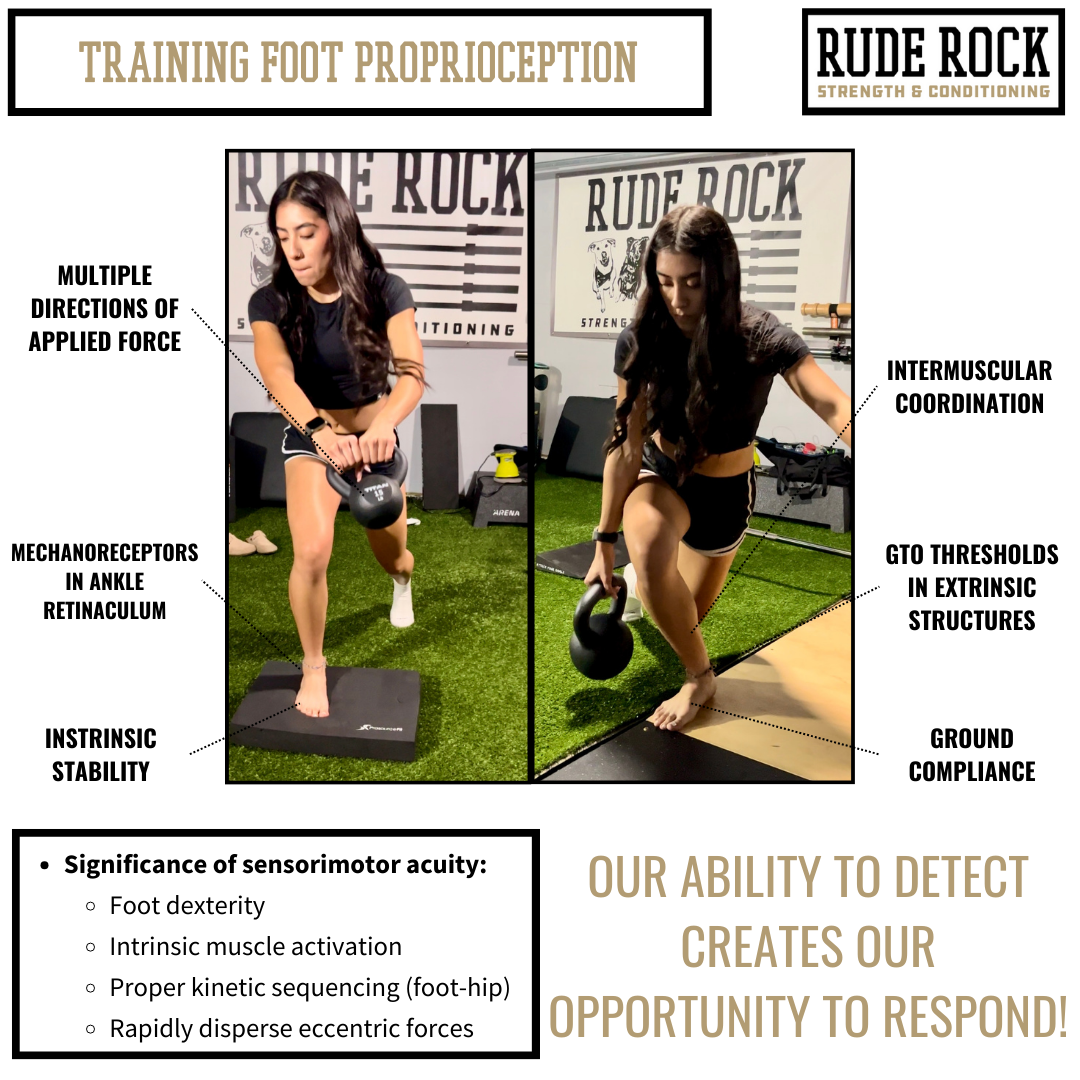
The ankle is a complex joint that adjoins the foot and lower leg by articulating the talus with the tibia and fibula bones. The ankle is classified as a hinged synovial joint as its primary actions include plantarflexion and dorsiflexion of the foot. However, unlike conventional hinge joints, the ankle has an array of movements outside of the sagittal plane to include inversion, eversion, medial and lateral rotation. Beyond the structural integrity provided by the retinaculum, it is highly enriched with sensorimotor bodies (i.e., proprioceptors & mechanoreceptors) that play a critical role in detecting joint positioning, force and velocity excursions, and relative body positions (5). It has been well documented that the proprioceptive acuity of the ankle retinaculum may be a primary factor for issues like chronic ankle sprains and midfoot sprains (5). Although structural integrity is a prominent consideration for ankle stability, proprioceptive acuity may be the primary factor for deterring ankle-foot injuries.
The foot itself is another sensory hotbed, as the plantar surface of the foot is one of the most densely layered tissues in the body for free nerve endings and proprioceptive bodies (4). As our feet interact with the ground, there is a kinetic response up the chain that stimulate specific muscular compartments depending on position of the foot, center of pressure, speed of movement, and position of the body. While there are obvious advantages to footwear, we have reached a point where functionality falls well behind fashion, and this has been consequential for the feet. For any athlete I work with, a forefront priority is to emphasize stimulating the sensorimotor bodies of the feet and improving proprioceptive acuity. This speaks to why I frequently have athletes out of their shoes for training. If proprioception is dormant, mechanical adaptations can be significantly more challenging to materialize and also predispose the athlete to maladaptive foot patterns or positions.
The Achilles tendon is the largest and arguably the most significant tendon in the body regarding athletic performance. Achilles tendon injuries have seemingly been on the rise across multiple sports, and when ruptured can be one of the most damming and challenging to return from. On a basic level the Achilles acts as a force absorber upon ground contact (eccentrically), and powerful force transmitter (concentrically) at toe off. The Achilles originates on the superior aspect of the calcaneus and inserts into the common tendon of the calf muscles, known as the triceps surae. This is an important aspect of the Achilles anatomy, as disproportionate development of the two gastroc muscles and the soleus can result in improper torque on the Achilles tendon. Another important consideration for Achilles anatomy is recognizing the adjacent posterior tibialis, which runs parallel to the Achilles on the medial aspect of the lower leg. The posterior tibialis is an extrinsic foot muscle that is primarily responsible for providing stability and support to the midfoot, while also assisting in plantarflexion and inversion of the foot. The posterior tibialis can informally be understood as the ‘sidekick’ to the Achilles, and when under functioning can contribute to chronic overloading of the Achilles tendon.
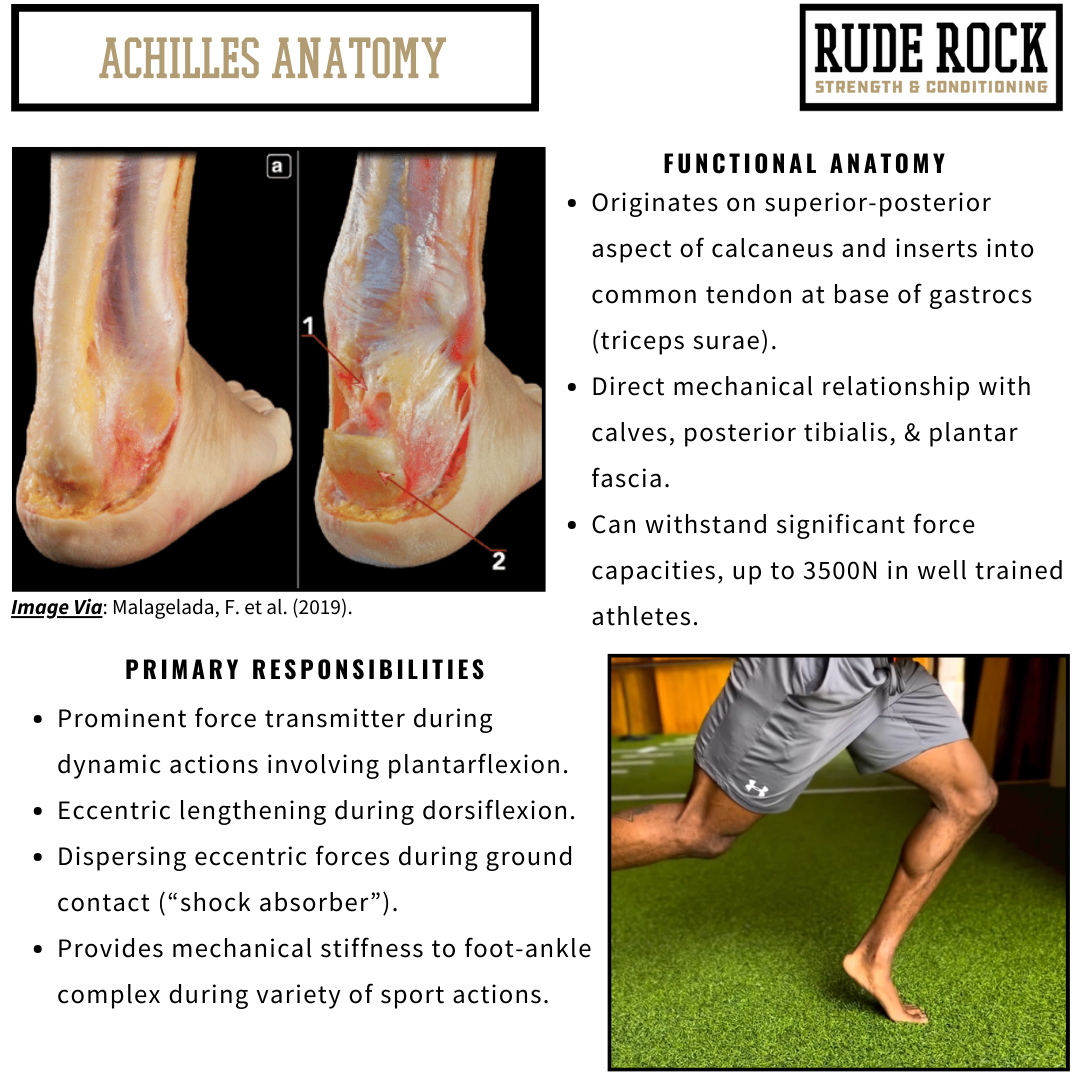
A lesser discussed aspect of the Achilles is the direct mechanical relationship it possesses with the plantar fascia. The significance of this mechanical relationship is wide-reaching, but it is rooted in the distribution of tension between the two adjacent tissues. For instance, an athlete who has chronically shortened (“tight”) calves will be somewhat more vulnerable for developing ailments such as Achilles tendinopathy due to excessive lengthening of the tendon. But what goes unrecognized is how this affects the positioning of the calcaneus, and therefore the tensioning on the plantar fascia. When the position of the calcaneus is disrupted due to tension-compression imbalances (i.e., pulled superiorly due to chronically tight calves), it can result in the plantar fascia being chronically lengthened and ultimately compromised in its functions.
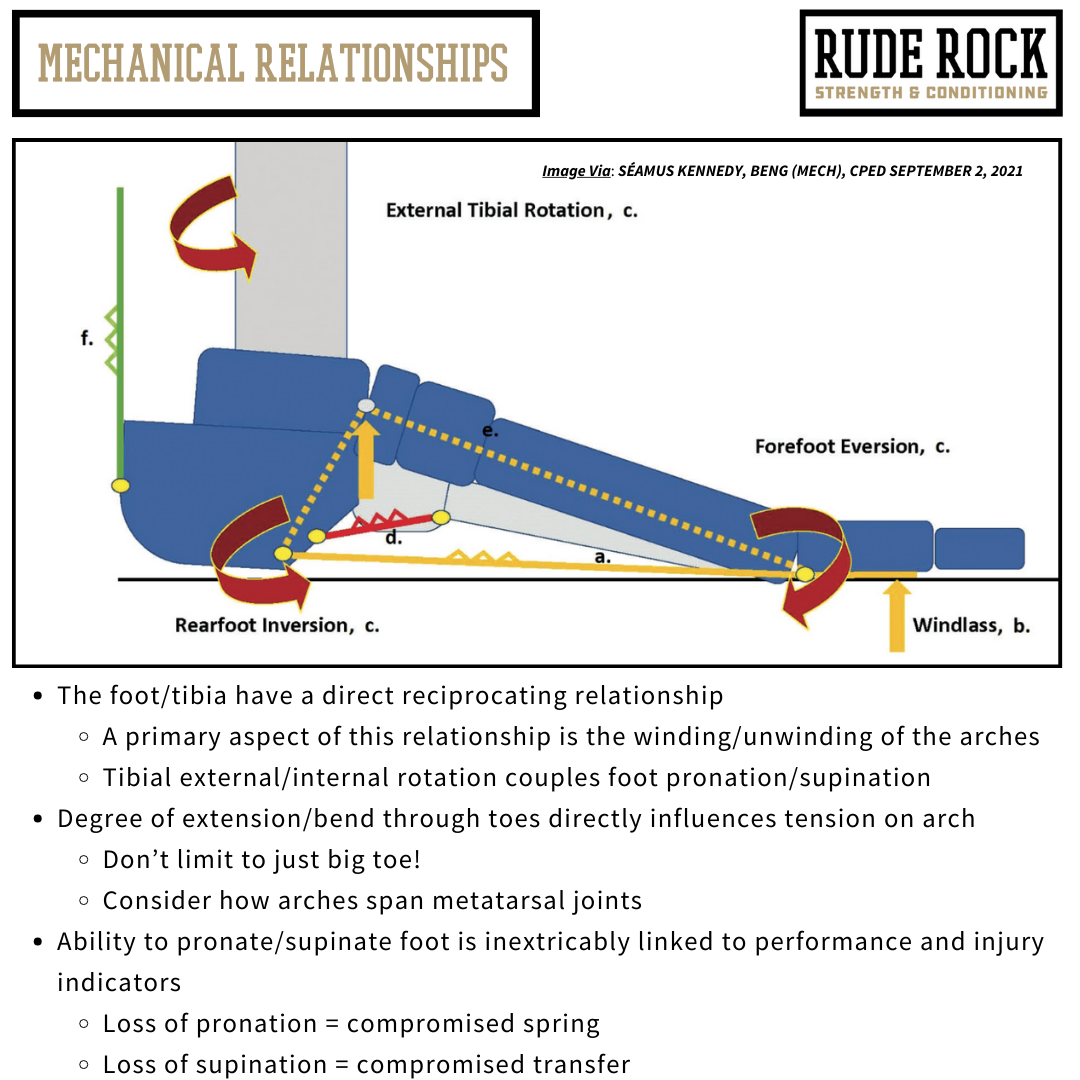
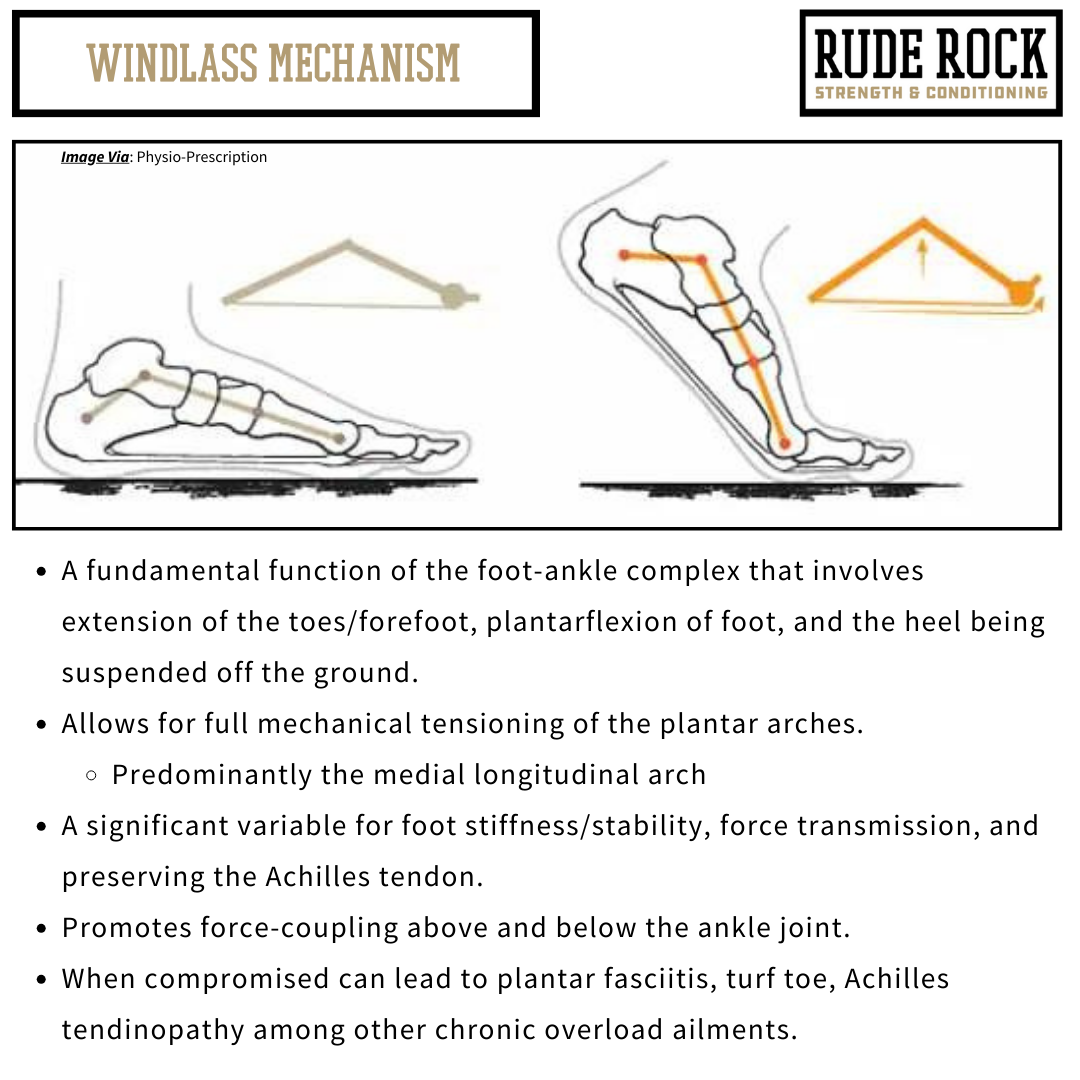
This relationship becomes magnified during the Windlass mechanism, which is a critical function of the foot-ankle complex that involves extension of the toes with concurrent plantarflexion of the foot. The Windlass mechanism is what allows the foot to create a mechanical locking of the midfoot to promote full tensioning of the medial plantar arch and allowing the foot to store and release mechanical energy. This is an action that is demanded in virtually any sport and is a significant factor for severe injuries such as Achilles ruptures, midfoot fractures, and plantar fasciitis.
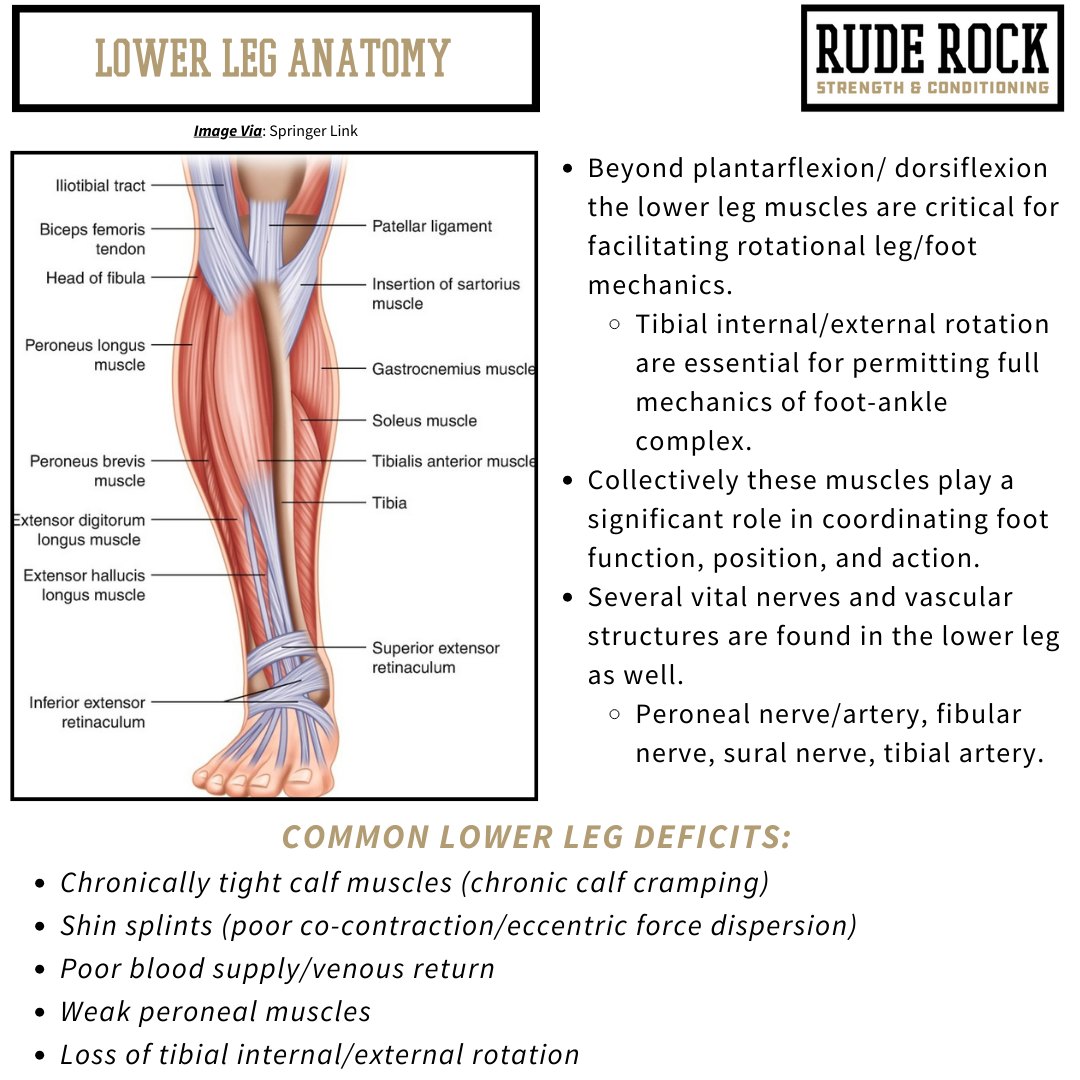
Finally, we have the anatomy of the lower leg, which can be simply classified as having four primary compartments- anterior, posterior, medial, and lateral. Each compartment possesses a significant role for foot-ankle function and requires specific modifications in training to be addressed appropriately. The two structures of the lower leg that I have found to be both commonly undertrained and highly valuable for athletes is the peroneal group and the aforementioned posterior tibialis. The peroneal group is collectively responsible for motor actions such as eversion, lateral rotation, and assists with plantarflexion. The peroneal group is collectively made up of the peroneus longus, brevis, and tertius, and although these function in tandem it’s important to recognize the independent actions of these three muscles. For example, where the peroneus brevis and longus cross the ankle joint on the posterior aspect, the tertius crosses anteriorly. Meaning, while the brevis and longus are responsible for plantarflexion actions, the tertius is a dorsiflexor of the foot.
Bringing it All Together
The anatomy of the foot-ankle complex can be difficult to fully grasp, as there are several structures and biomechanical actions to be aware of. The most important thing to grasp, at least initially, is recognizing the inherent mechanical relationships and reciprocating function of the foot-ankle complex. Beyond that, understanding the primary functional compartments of the foot and lower leg can help coaches become better informed for decision making and problem solving with their athletes. Being proficient with foot-ankle anatomy doesn’t require you to be able to recite each and every structure that is involved, but more so being aware of the primary anatomy structures and more importantly being able to understand how these structures relate to and influence the complete body.
This article was published as a preliminary piece to set the stage for subsequent articles to follow. If you enjoyed and found value in this article, please do us the kind favor of sharing with your peers, athletes, and friends. And then stay tuned for follow-up articles coming discussing how this anatomy can be applied in a practical sense.
References
1.) Bates KT, Collins D, Savage R, McClymont J, Webster E, Pataky TC, D’Aout K, Sellers WI, Bennett MR, Crompton RH. 2013. The evolution of compliance in the human lateral mid-foot. Proc R Soc B 280: 20131818.
2.) Card RK, Bordoni B. 2023. Anatomy, Bony Pelvis and Lower Limb, Foot Muscles. StatPearls.
3.) Chan, CW. Rudins, A. 1994. Foot biomechanics during walking and running. Mayo Clin Proc, 69:448-461.
4.) Fahradyan, A. Patel, KM. 2020. Essential anatomy of the lower leg. Handbook of lower extremity reconstruction: Springer Link. 13-42.
5.) Fraser JJ. Feger, MA. Hertel, J. 2016. Midfoot and forefoot involvement in lateral ankle sprains and chronic ankle instability. Part 1: Anatomy and biomechanics. Int J Sport Phys Ther. 11:6.
6.) Udofa, A. Ryan, L. Clark, K. Weyand, P., 2017. Ground reaction forces during competitive track events: a motion based assessment method. Intl Soc Biomec in Sport.
