
Rude Rock Field Guide to Tendon Pathology
Tendon pain is extremely common, however sometimes the complexity of the disease is often overlooked. Of course being more prevalent in athletic populations, the fact of the matter is, anyone can have tendinopathy from overuse. I'm sure most of us reading this have dealt with some form of tendon pain one way or another, but for a lot of folks, tendon pain can be very debilitating. And for some of us, debilitating can be a huge understatement.
In this “field guide”, we won’t get into specific treatments, therapeutic exercise techniques, strength programming, or load management techniques. Instead, the aim of this article is to give the reader a better understanding of the pathophysiology of tendinopathy from a 10,000ft view. Giving coaches and young clinicians a more concise explanation and synthesis on how tendons behave when pathologic. Tendinopathy is a major problem with extremely active individuals and sports populations. With the complexities that come from tendinopathy, the more complex issues can arguably be finding the best treatment and training program methods in resolving the issue. So why is tendon pain or tendinopathy a lot more complex than we realize? It’s because it’s not a definitive singular disease.1 The problem lies in the evolving nature of the body’s ability to keep up with its healing response. The clinical condition is a very long continuum of events that shift based on variables of the internal and external environment.2 What we do as coaches and clinicians can affect how our athlete’s tendon pain behaves and change its pathologic characteristics for better or for worse at various stages. This is why, with so many clinical treatment options and strength programming strategies and methodologies that are available, it seems that in some cases, it can appear like nothing seems to work.1 Case and point, our treatments and strength program effectiveness can arguably be dependent upon where on the continuum the athletes tendon healing lies.
With tendinopathy under the umbrella of “overuse” injury, the clinical manifestation of its chronicity can be defined by the inability for the body to sustain an optimal healing response. Once mechanical loading of a tendon is introduced, the cellular matrix response takes 2 paths: adequate or inadequate.1,2,3 If the cellular matrix considers load as adequate, then positive training adaptation will occur making our healing response within normal limits and allowing our tendons to become stronger and heal adequately for the next intensive bout. If the cellular matrix considers the training stimulus or load to be inadequate, then there is a slight window of momentary weakness. With this transient window of tendon weakness, if the athlete continues to repetitively load the tendon and continues to exceed the body’s capability of healing and achieving homeostasis, that is where injury occurs. With repetitive load and excess of that load overtime, it becomes overused. So overall, it’s an imbalance of cellular matrix degeneration and synthesis. Tendinopathy being a net negative balance of degeneration. In extreme situations, from a cellular picture, Kader et al 20024 described tendinopathy as a non-inflammatory, intratendinous collagen degeneration with fiber disorientation and thinning, hypercellularity, scattered vascular ingrowth and increased glycosaminoglycans.1,4
TENDON STRUCTURE
We’ll visit the clinical hierarchy of tendon structure and cellular mechanobiology. However I would be remiss to not mention the direct role of the fascial system when it comes to tendons in general. If you’re not familiar with Rude Rock’s intensive involvement in studying the fascial system, I encourage you to seek our educational outlets to learn more about the fascial system. But in a nutshell, the fascial system is a three dimensional continuum of tissue containing collagen, loose and dense fibrous connective tissue, permeating the entire body, endowing the body with a functional structure, that provides the environment to enable all body systems to operate in an integrated manner.6,7 With the many elements incorporated within the fascial system pertaining to biomechanics and pain generation, specifically myofascial expansions; which have sophisticated origins and insertions between aponeurotic fascia and skeletal muscles and tendons;6 the need to highlight this is to inform readers that tendons and tendon health are also within the seamless nature of the health and adaptive response to our fascial system. However what I don’t want to create is the impression that this information in this article is incomplete, but to highlight the objectivity of what is going on, on the cellular level of different phases in the tendon structure in pathologic tissue.
It's commonly known that tendons proper, are what connect muscle to bone both proximally and distally. With the muscular attachment being the myotendinous junction (MTJ) and the bony attachment being the osteotendinous junction (OTJ). Tendon’s role is for force generation and transmission to elicit skeletal movement, or simply a mechanical bridge.8The shape and size of a tendon is dependent upon the role of the muscle’s power and force generation in both isolated and compound gross movement.
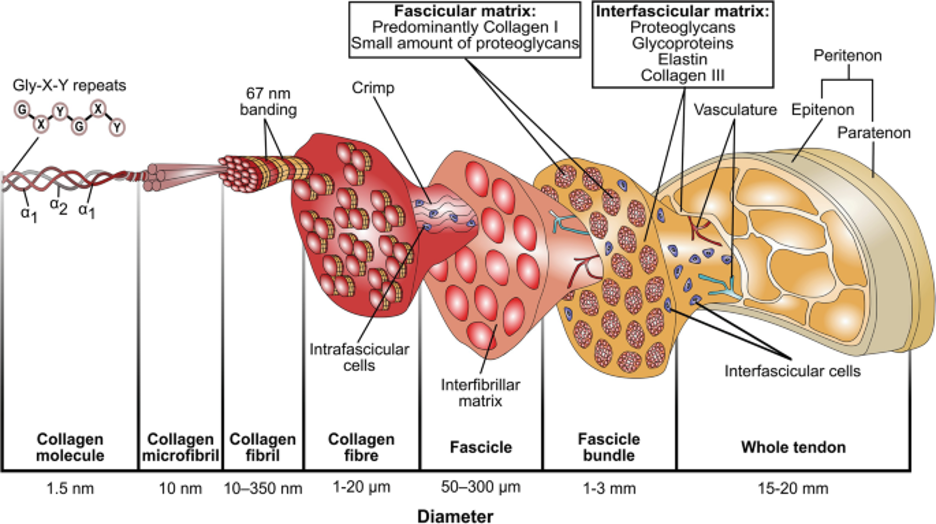
The image below gives a visual representation of the structural hierarchy of the tendon’s collagen strands.9
Lets dive into the cellular and non cellular components of the tendinous environment. We can think of the entire tendon covered in sheaths. Bordoni and Varacallo10 describe tendon anatomy as follows: Tendon sheaths are structures that aid in the smooth gliding movement of tendons between neighboring structures. Fibrous sheaths, or more commonly referred to as retinacula, serve as channels for tendon movement for long tendons. They prevent significant friction and irritation on neighboring tissues at bone structures, ensuring smooth sliding and gliding action. Synovial sheathsfacilitate tendon sliding within the fibrous sheath. These structures enclose a space with peritendinous fluid that serves mainly as a lubricant. True synovial sheaths are only found in areas necessitating highly efficient lubrication due to sudden direction changes and increased friction. Peritendinous sheets have overlapping functions with the synovial sheaths despite having cellular differences. The paratenonium (or paratenon) is composed of type I and type III collagen fibrils and thin elastic fibers. This paratenon reduces friction and works like an elastic sleeve, allowing free tendon movement within its environment. Reflection pulleys are thickened regions of dense fibrillar tissue found within fibrous sheaths, encasing tendons within the sliding bed, particularly around tendon curves. Reflection pulleys facilitate smooth tendon movement. Deep to the paratenon, the entire tendon is surrounded by a thin, dense connective tissue sheath called the epitenon. The paratenon and epitenon are collectively called peritenonium. Collagen fibrils within the epitenon are oriented transversely, longitudinally, and obliquely. The epitenon fibrils occasionally appear fused with the superficial tendon fibrils. The epitenon is connected to the peritenonium externally and endotenon internally. The endotenon, a thin membrane, covers and organizes individual tendon fibers into larger units bundled in various orders. This membrane separates different collagen bundles, allowing neurovascular penetration within the tendon.
Within the tendon’s cellular components, the fibroblasts that contribute to the formation of its tendon tissue primarily include tenocytes (which are mechanosensitive cells) and tenoblasts. Tenoblasts represent approximately 90% to 95% of tendon fibroblasts. These specialized fibroblasts produce extracellular matrix components (ECM),11 which include collagen and proteoglycans (more structural support for the ECM). Collagen makes up approximately 65% to 80% of the extracellular matrix. The predominant collagen type in tendons is type I. Type III collagen is present in the epitenon and endotenon. Type II collagen occurs in the osteotendinous junction's fibrocartilaginous areas. Elastin, proteoglycans, and glycoproteins constitute 4%, 4%, and 2% of the extracellular matrix, respectively.10
The blood supply of tendons can be split between the intrinsic and the extrinsic.8 The intrinsic sources are at the MTJ and the OTJ, while the extrinsic sources are at through the paratenon or the synovial sheath.8 The blood supply to specific areas is supplied by different sources. The intrinsic at the MTJ has been documented to extend into 1/3 of the tendon whereas the blood supply originating from the OTJ is more avascular and is limited to the insertional point.8 This leaves the extrinsic source to supply the mid portion of the tendon.8
TENDON INJURY REPAIR & DYSREPAIR
The severity of tendon damage is dependent on the magnitude of overuse. From a predisposition standpoint, age, biological sex, and genetics can be factored in.1 As we age, connective tissue and tenocyte quality diminishes, females may be more prone to tendon inflammatory responses and healing responses, and some genetic markers that are more pro inflammatory can be more prominent. Additionally in less common cases, systemic predispositions may include certain proteins that help control inflammation may not be as abundant, high cholesterol levels can cause tendon pain, diabetes, and certain drugs; specifically some families of antibiotics can cause tendon pain.1
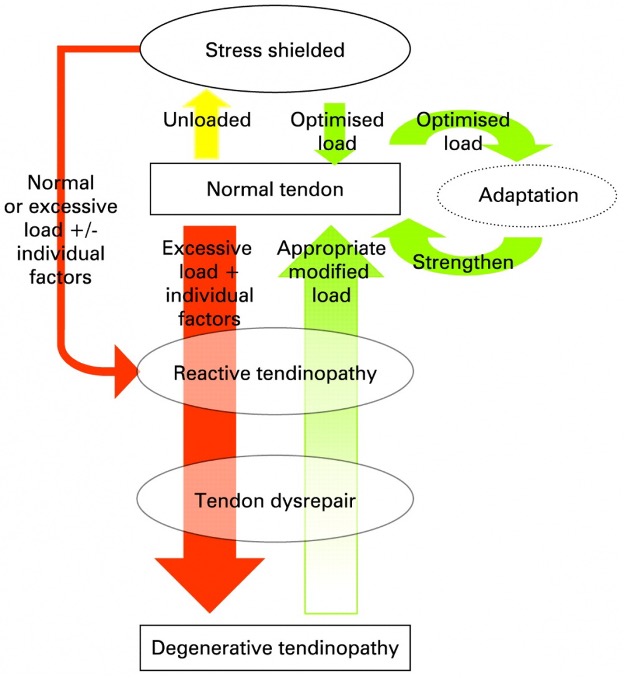
Because of our understanding of the tendinopathy continuum, our approach in selection of intervention for therapeutic repair are directly dependent on the severity of tissue damage and the ability for the tendon to respond to therapeutic stimuli. The less damage that is present, the increase of potential reversibility of the disease. Going back to Cook and Purdum’s tendon continuum they proposed 3 stages within the continuum being 1. Reactive Tendinopathy 2. Tendon Dysrepair and 3. Degenerative Tendinopathy.1,2,3,4,5 Respectively, we can visualize these stages on a green yellow red scale and how well we are either moving the needle towards the green and exciting more healing response or moving the needle towards red approaching increased degeneration and potential rupture.1 Green is optimal repair where tendons have the ability to repair themselves. These are the instances where rest and decrease in repetitive stress and force is enough to heal back to 100%. Yellow being failed repair stages where there is still the ability and potential for reversibility of the disease. The yellow area can be a bigger margin, either being closer to green where less invasive measures of treatment and training options can be enough to push the tendinopathic tissue to the green zone, or even closer to the red zone where naturally we would need more sophisticated treatment options to kickstart better healing responses that our body simply can't do by itself.1 Finally red being a failed tendon healing response that is more often irreversible.
The first stage is reactive tendinopathy defined by a non-inflammatory proliferative response from alterations in the cellular matrix.1,2,3,4,13,14,15 This is more commonly resulting from compressive or tensile overload.4,13,14 We may see tendon thickening due to the changes in the ECM as a reaction to a sudden and unprepared increase of stress.3 On a cellular level, it’s common in this phase to see the tendon tissue changing to appear more cartilaginous in nature (cell metaplasia).1 We see proliferation of less durable collagen and formation of new vascular networks (neovascularization) in an attempt for the tendon to heal.14 There’s separation of collagen fibers and fibril damage, and an increase in pro inflammatory mediators.1,2,4,12,14,15
The tendon dysrepair stage is the progression of reactive tendinopathy with increased ECM damage and disorganization of repair.1,12,13,14 In this stage, the tendon tissues are less metabolically active and more catabolic due to the cells being even more cartilaginous, which makes the tendon less receptive to healing factor stimuli.1 There’s an increased proliferation in vascularity with ingrowth of blood vessels from existing blood vessels (neoangiogenesis) and proliferation of nociceptors that detect and react to noxious stimuli and mechanical pain of disorganized healing.1,12,13,14,15 In this stage, radiographic imaging can show that there are changes in the tendon.3 Tendon dysrepair can be tame or severe, again being more towards the green or the red. This is where load, force, and volume management in activity are important to potentially see the irreversible effects on the continuum.
The degenerative tendinopathy stage is now the irreversible stage of tendinopathy with significant ECM breakdown and negative morphology in its tissue properties. Here we have extreme ECM degeneration, programmed cellular death (apoptosis), and not enough anabolic cells to build and repair.1,12,13,14,15, 16 This tendon is extremely fibrotic which may require more sophisticated measures of therapy or surgical intervention. In these later stages of tendinosis, the proliferation alone can be so vast, which may explain why platelet rich plasma injections (PRP) don't respond at all to healing mechanisms.1,17
The image below can give us a visual of these ingrowths within the tendon that change its tissue characteristics and allow for a vicious cycle of pain behavior patterns.18,19
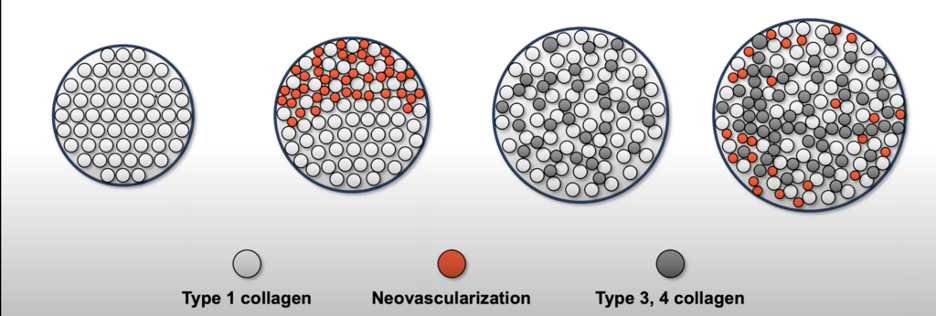
As you can see from this illustration of a cross sectional diagram, diseased tissue is a mixed bag of cellular ingrowth from what our body tries to heal.1,18,19 The caveat to all this, is that this occurs because of the body’s lack of a true inflammatory response due to small micro traumas that don’t correctly signal an appropriate acute healing response we need.1,19 Hence the “non-inflammatory proliferative response”. This explains why NSAIDS may not work either.1,20
There are a lot more things to consider well beyond this “field guide”, but past the predispositions an individual may have to tendinopathy in general, the biomechanics of tendons can also add additional nuances to how tendons behave to stimuli. For example, certain tendons under various loads at precise angles can hyper load very specific parts of a tendon, certain tendons may have more vascularity than others, and some tendons may or may not have better abundance of healing cells.1,14
For any healing to occur, we must always aim to place our bodies in the most optimal healing environment. The simplicity of understanding load management, optimal stimulation of ECM activity, activating anabolic enzymatic production while minimizing pro-inflammatory mediators, and decreasing neovascularity are the keys for placing tissue in that optimal healing environment and allowing tendons to heal.1 Unfortunately, the complexity of the disease continuum makes it easier said than done. Not a single treatment can work all of the time, based on where the healing environment is at. It may take simultaneous treatment options in a given moment to illicit desirable healing responses. But even then, those responses can vary. What may work for many may not work for certain individuals and vice versa. Which all together, can make management an extremely daunting task. As we continue to understand this continuum as well as understand the characteristics and behaviors tendons can present, let this field guide simply be the start of us continuing to seek research and acquiring more tools in our tool box in how we can better manage tendinopathy with our athletes.
References:
1. Husky Orthopaedics. Basic Science Rationale for Current Treatment Algorithms for Tendinopathy. YouTube. Published June 7, 2018. Accessed August 22, 2024. Basic Science Rationale for Current Treatment Algorithms for Tendinopathy
2. Cook JL, Rio E, Purdam CR, Docking SI. Revisiting the continuum model of tendon pathology: what is its merit in clinical practice and research? British Journal of Sports Medicine. 2016;50(19):1187-1191.
3. Lee M. Tendon Pathophysiology. Physiopedia. Published 2015. https://www.physio-pedia.com/Tendon_Pathophysiology
4. Kader D. Achilles tendinopathy: some aspects of basic science and clinical management. British Journal of Sports Medicine. 2002;36(4):239-249. doi:https://doi.org/10.1136/bjsm.36.4.239
5. Lee M, ed. Tendon Continuum.; 2015. Accessed August 22, 2024. https://www.physio-pedia.com/Tendon_Pathophysiology
6. FASCIAL MANIPULATION INSTITUTE by STECCO. Myofascial Expansions-English Version. YouTube. Published September 22, 2022. Accessed August 16, 2024. Myofascial Expansions-English Version
7. Stecco A, Giordani F, Fede C, Pirri C, De Caro R, Stecco C. From Muscle to the Myofascial Unit: Current Evidence and Future Perspectives. International Journal of Molecular Sciences. 2023;24(5):4527. doi:https://doi.org/10.3390/ijms24054527
8. Physiopedia. Tendon Anatomy. Physiopedia. Published 2012. https://www.physio-pedia.com/Tendon_Anatomy
9.Tendon Extracellular Matrix Assembly, Maintenance and Dysregulation throughout Life | SpringerLink.; 2021. Accessed August 20, 2024. https://www.google.com/url?sa=i&url=https%3A%2F%2Flink.springer.com%2Fchapter%2F10.1007%2F978-3-030-80614-9_3&psig=AOvVaw3B03nQDQ76xW_kQeq7oTPu&ust=1724445987903000&source=images&cd=vfe&opi=89978449&ved=0CBcQjhxqFwoTCPizusa8iYgDFQAAAAAdAAAAABAE
10. Bordoni B, Varacallo M. Anatomy, Tendons. Nih.gov. Published April 7, 2019. https://www.ncbi.nlm.nih.gov/books/NBK513237/
11. Frantz C, Stewart KM, Weaver VM. The Extracellular Matrix at a Glance. Journal of Cell Science. 2010;123(24):4195-4200. doi:https://doi.org/10.1242/jcs.023820
12. Leadbetter WB. Cell-matrix response in tendon injury. Clin Sports Med. 1992 Jul;11(3):533-78. PMID: 1638640.
13. Base NRC (US) SC for the W on WRMITR. Response of Muscle and Tendon to Injury and Overuse. National Academies Press (US); 1999. https://www.ncbi.nlm.nih.gov/books/NBK230857/
14. Wang JH-C, Guo Q, Li B. Tendon Biomechanics and Mechanobiology—A Minireview of Basic Concepts and Recent Advancements. Journal of Hand Therapy. 2012;25(2):133-141. doi:https://doi.org/10.1016/j.jht.2011.07.004
15 .Järvinen TA. Neovascularisation in tendinopathy: from eradication to stabilisation? British Journal of Sports Medicine. 2019;54(1):1-2. doi:https://doi.org/10.1136/bjsports-2019-100608
16. Killian ML, Cavinatto L, Galatz LM, Thomopoulos S. The role of mechanobiology in tendon healing. Journal of Shoulder and Elbow Surgery. 2012;21(2):228-237. doi:https://doi.org/10.1016/j.jse.2011.11.002
17. Andres BM, Murrell GAC. Treatment of Tendinopathy: What Works, What Does Not, and What Is on the Horizon. Clinical Orthopaedics and Related Research. 2008;466(7):1539-1554. doi:https://doi.org/10.1007/s11999-008-0260-1
18. King D. Tendinosis and the Role of Minimally Invasive Tenotomy. Accessed August 20, 2024. https://www.youtube.com/watch?v=erjvcu01z4A
19. TenJet HydroCision Inc. Tendinosis and the role of Minimally Invasive Tenotomy. YouTube. Published November 9, 2022. Accessed August 22, 2024. Tendinosis and the role of Minimally Invasive Tenotomy
20. Andres BM, Murrell GAC. Treatment of Tendinopathy: What Works, What Does Not, and What Is on the Horizon. Clinical Orthopaedics and Related Research. 2008;466(7):1539-1554. doi:https://doi.org/10.1007/s11999-008-0260-1
