
Training Considerations for Knee Pain
While the knee is a relatively simple joint, paradoxically, it can be a difficult joint to navigate in training- especially when pain or injury are present. The knee, a modified hinge joint, is a sagittal-based joint that works predominantly through flexion/extension patterns. A common perspective for analyzing the functional role of the knee is by viewing it as the biproduct of the hip and the foot. Although this obviously isn’t entirely thorough, there is a good bit of truth to this and at the least can be a good starting point for young coaches. The primary factor to consider when analyzing the relationship between the foot/knee/hip is understanding torque and the responsibilities each joint has to manage it. Torque, which is the summation of force and moment arm, or in simple terms- rotational force, is not favorable for the knee. Nevertheless, torque demands will ultimately be the rate limiting factor for knee health.
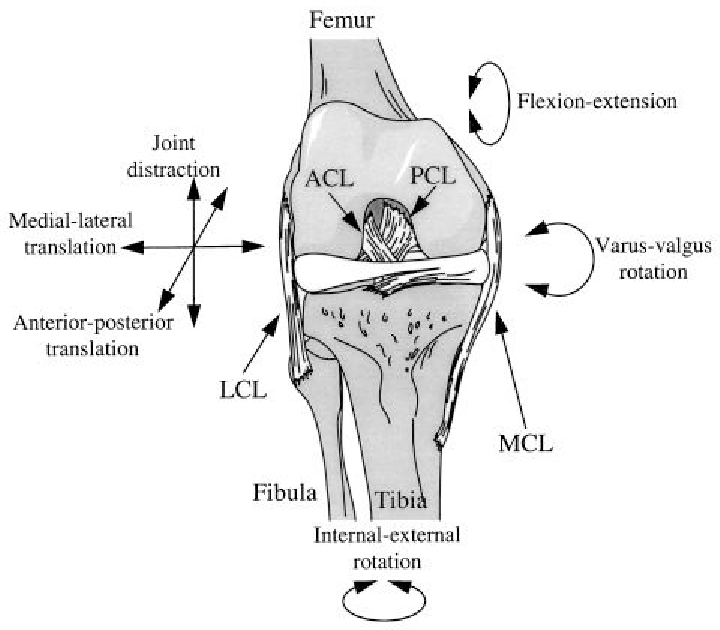
Where the foot (ankle) and hip are more fundamentally designed to accommodate torque, the knee is not. The reason being, these are joints that are designed to move in multiple planes of direction, or multiplanar. A reduction of mobility at the hip, namely internal/external rotation, and/or a reduction in stability at the foot, will cause the knee to take on more responsibility as a torque converter. When this occurs, pain and problems will almost certainly manifest at the knee joint.
General Approaches to Injuries Before we get into the details of working around knee injuries, there are some common variables I subscribe to when working with any injured athlete, irrespective of joint or injury type. In my opinion, looking at exercise or specific exercise selection as binary options is a reductionist approach. Sure, there are obvious cases like an athlete with severe disc compressions and their candidacy for back squats… but beyond the obvious, I think most items should be viewed as “how” not “if”. There are four primary variables to look at when assessing someone’s eligibility for optimal movement. Those being:
I.) Range of motion
II.) Path of motion
III.) Load
IV.) Speed
We’ll use a squat for an example here. Let’s say someone is having difficulty getting to 90 deg., whereby the closer they get to a parallel squat, the more pain they’re getting unilateral knee pain. Rather than just simply saying “ok squats aren’t going to be a good option”, I want to work through the variables outlined above as regressive tiers.
I.) Have the athlete stop just before the presence of pain; use box if needed
II.) Ensure that they are starting from and initiating the movement through a good hip/hamstring dominant pattern (also analyze foot position, width, & trunk angle)
III.) Reduce the load or change the placement of the load
IV.) Slow the entire movement down, apply tempo schemes (i.e., eccentric-iso)
There are obviously several variables at play when considering training around pain, but if you isolate those four variables and follow the appropriate regression-progression scheme, you will put the athlete in a position to succeed more often than not. Some additional primary ones that I feel are important to recognize:
Contraction Type: There’s a great deal of difference between eccentric and concentric muscular actions. For the sake of pain and injuries, pain/discomfort during the eccentric phase of movement (muscular lengthening) is normally more indicative of tendinous/joint capsule issues. Conversely, pain during the concentric action typically corresponds to more muscular/motor control problems. During the eccentric phase, the tendinous junctions are placed under high levels of stretch as the muscle is being forcibly lengthened under load. Tendons are also responsible for absorbing and storing energy to be utilized during the stretch reflex. So, someone with tendinous pain may be good to squat heavy but must move slow and perhaps in a partial ROM. An athlete with a muscular strain, conversely, may be able to move at normal speed and in full ROM, but will inherently be limited by intensity.
Muscular Sequencing: Kinetic or muscular sequencing is paramount for fully amending injuries. A simple one to point out is the “1/2/3” firing for hip extension, where the glute (1), hamstring (2) and contralateral QL (3) fire in that order to achieve the movement. Having a disruption to muscular sequencing, very common following injury, means that muscles are doing more or less work than they typically should. This not only compromises ability or capacity but can also place undue stress on the surrounding joints.
Volume or Intensity: The two training parameters that ultimately govern any program are volume and intensity. Depending on the training goal and the ability and health status of the athlete, these parameters must be fluctuated accordingly. With regard to injuries, acute injuries will normally occur due to excessive intensity, whereas chronic injuries are usually more a consequence of excess volume. In either case, both must be managed appropriately when working with injured athletes, remember, the difference between poison and medicine is dosage and frequency.
1>0: A final point to address here is simply intent. Injured or not, the most vitally overlooked training parameter is intent, and this falls squarely on poor coaching. As we know quality trumps quantity in almost any situation, but with injured athletes, it couldn’t be any more significant. Consider the 1>0 theory here like this: a quality rep of just about anything is more redeemable than countless reps of something done poorly. The instruction for the athlete needs to be precise, and the execution deliberate.
Knee Pain and Injuries
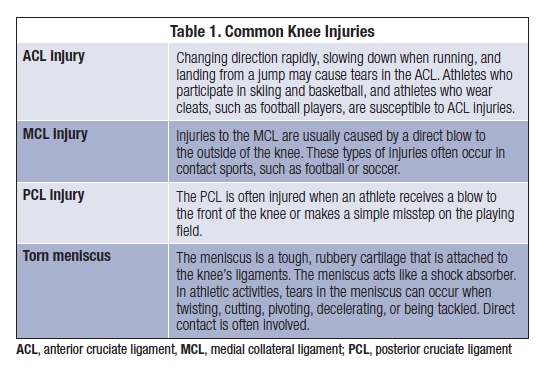
There are a host of common knee injuries in the athletic realm, and each injury presents a specific subset of parameters to be aware of. Considering I don’t want to turn this into an injury literature review, the graphic to the left summarizes the mechanism of common soft tissue injuries. In addition to the chart above, some other common knee injuries include arthritis (degenerative joint cartilage), tendinitis (quad, patellar or IT band), and bursitis. While the ones outlined above are generally more acute-based injuries, these three speak more to the chronic side. As we know chronic injuries typically manifest through overuse, poor mechanics, or simply demands of sport/duty. But in either case, as we can see almost all major knee injuries involve soft tissue structures (i.e., ligaments & tendons). There are some notable differences with how we should prioritize or progress athletes depending on whether we’re dealing with a ligamentous or tendinous injury. And again, we can isolate and manipulate just a few standard training parameters to ensure we’re putting the athlete in the best position possible.
Basic Knee Mechanics
As I mentioned the knee can be tricky to work around, despite the simplicity in its functional roles. In an effort to reduce the ambiguity, I use a few broad “markers” that I tend to abide by when dealing with knee pain:
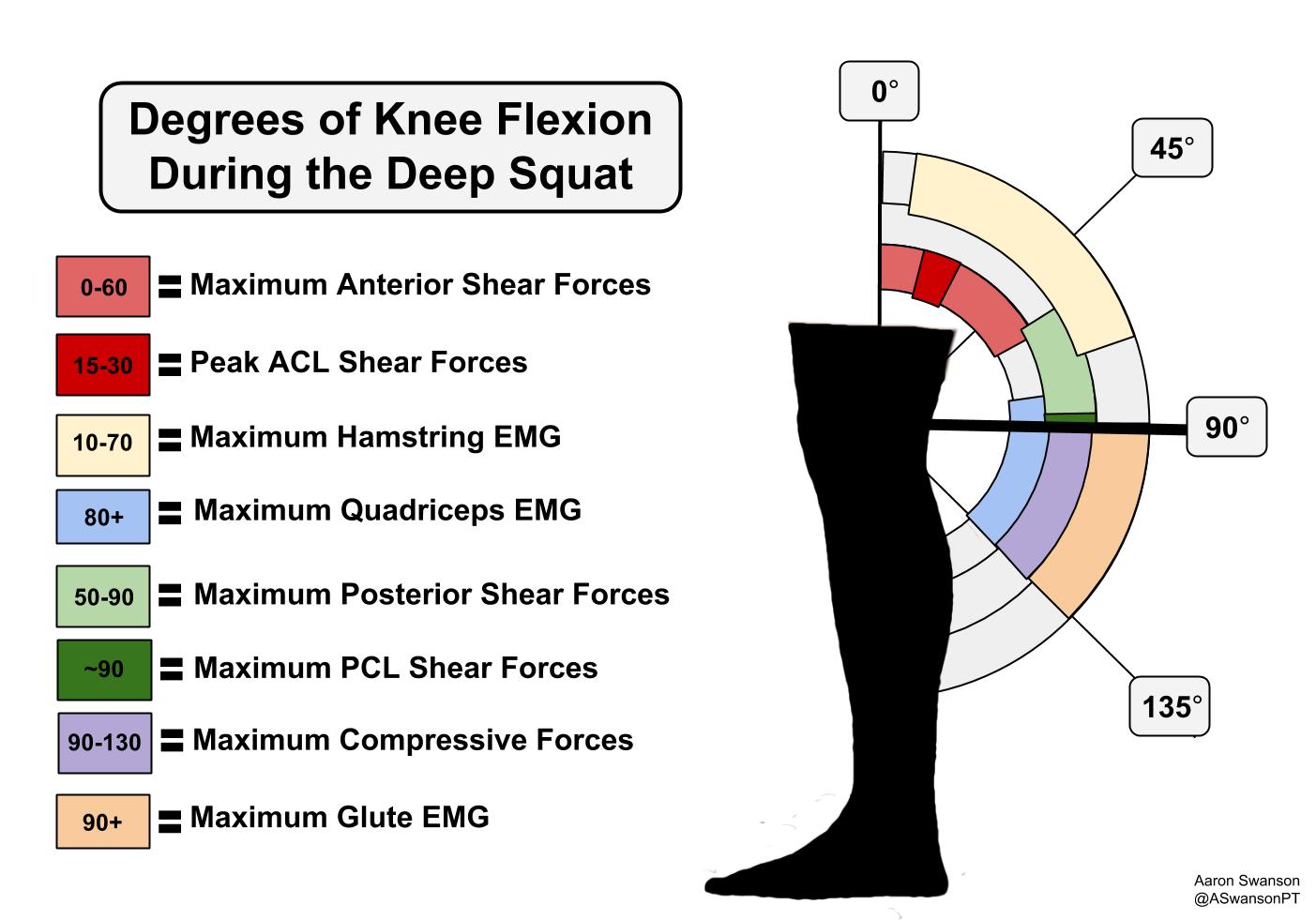
I.) Above 90 = Quad tendon & ACL stress zone (10-30 specifically for ACL)
-->Max anterior shearing forces
II.) Below 90 = Patellar tendon & PCL stress zone (90-120 specifically for PCL)
-->Max compressive forces
III.) At or Below 90 = meniscus stress zone (much more variability w/ meniscus)
Increased varus/valgus force = LCL/MCL stress zone
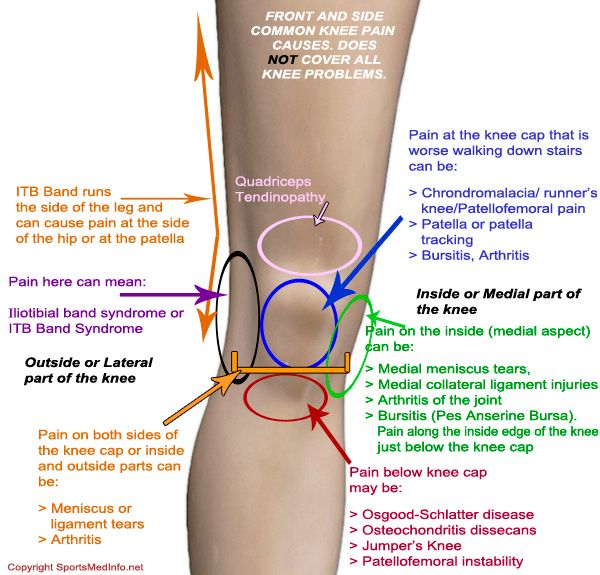
Along with the specific ranges of motion, we can also look at referred and localized pain sites as well. While this is not something inherently consistent across all individuals, it can be helpful especially when a formal diagnosis hasn’t been established. The image below shows the common pain sites and what those pain sites can indicate. Again, this is a good image to be familiar with and can help with troubleshooting pain patterns and putting athletes in safe positions.
Training Considerations
Accommodating for knee pain during training will be focused mostly on the joints above and below. One thing a lot of individuals overlook is that knee mechanics (and forces) can be wildly modified by simply adjusting position and stance. For instance, just the amount of dorsiflexion (DF) alone can dramatically change the outcome of a squat pattern and subsequent knee pain. The primary effect with amount of DF is how it influences the moment arm (i.e., torque) experienced at the knee. When athletes cannot adequately dorsiflex, it forces the hips and lumbar to move through a restricted path of motion causing a disruption in how the force is distributed throughout the body. Consequentially, there is a greater discrepancy between knee and hip flexion, which substantially increases the presence of shearing force at the knee.
Essentially, you want to play with the demands placed on the hips and positioning of the feet to “find the sweet spot” for the knees. In addition to the general factors listed above (ROM, POM, Load, Speed), there are three things I like to address with athletes battling knee pain:

I.) Torso and shin angles should be mirrored
Trunk inclination itself is a highly influential factor for knee stress/demand. Increasing the amount of trunk flexion during squatting primarily does two things for the athlete, first, creates a shorter moment arm thus {theoretically} reducing the amount of torque experienced at the knee. And secondly, it places less demand on the rectus femoris as a knee extensor because it is working more in hip/trunk flexion.
When I say “mirror the trunk and shin angles” what I believe this does is creates more appropriate alignment (i.e., keeping center of mass atop midfoot center of pressure) for the athlete as they move through their pattern. As a result, forces are more appropriately distrusted between muscles crossing both the hip and the knee joints. In addition, this seems to indirectly help with improving kinetic sequencing, as the movement pattern is more fluent throughout. For healthy athletes, I like to have a knee over toe pattern with slight trunk flexion. This obviously isn’t cut and dry, as a number of variables are at play, but in most cases I find that to be optimal.
For athletes affected by injury, I will either have them exaggerate the knee over toe + trunk flexion pattern or have them keep a perfectly vertical shin with an upright torso. Generally speaking, pain above knee = knee over toe, pain below knee = more upright and vertical shin.
II.) Foot position/stability
Honestly, this could be a full article in itself but in an effort to keep this short and sweet, let’s look at the big picture. A reduction or insufficient foot stability will primarily affect the knee by increasing the presence of varus/valgus stress (recall- excess varus/valgus = bad for ligaments and cartilage). When we see athletes with poor pronation-supination control in the foot, there’s an accompanying shift in the amount of internal/external rotation placed on the tibia. The outcome being the knee is now exposed to shearing stress as it becomes more responsible to accommodate medio-lateral forces. This, over time, can create damaging consequences.
Along with providing a firm base of stability, the foot is also a major component to the proprioceptive system. When proprioception is compromised the body essentially has a reduced ability to detect and process environmental conditions, and with that comes a reduction in muscular firing rate, capacity and stretch. Collectively, when proprioceptors underperform, muscles (and thus, ligaments/tendons) are forced to endure more undue stress, making the joint more vulnerable to injury. Improving foot proprioception is a strong variable in solving the knee pain conundrum. If we can improve the proprioception of the foot, the muscles of the lower leg are more adept to fire and help stabilize the knee.
III.) Where the load is placed
If you’re not too familiar with how influential lever systems are with regard to human movement, I recommend you start here- Squat Levers. I will say lever systems can be a little difficult to fully grasp for young coaches but if you don’t know anything else, please know that they matter, greatly. For instance, a quick fix for minor “nagging” knee pain is to simply adjust where the athlete places the load.
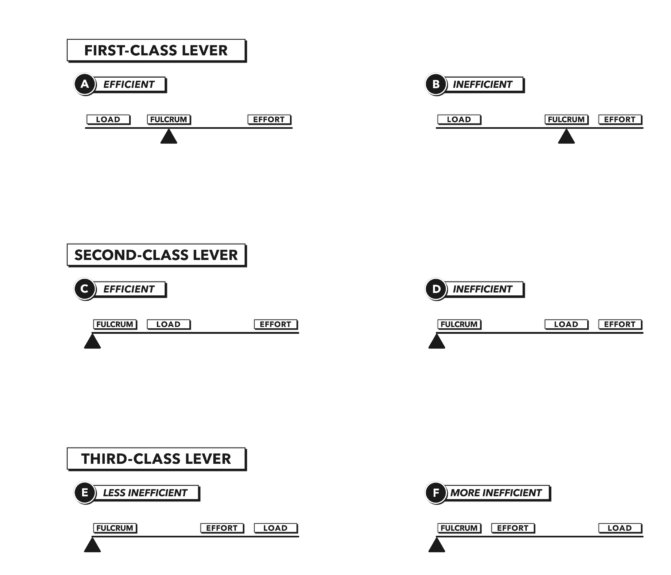
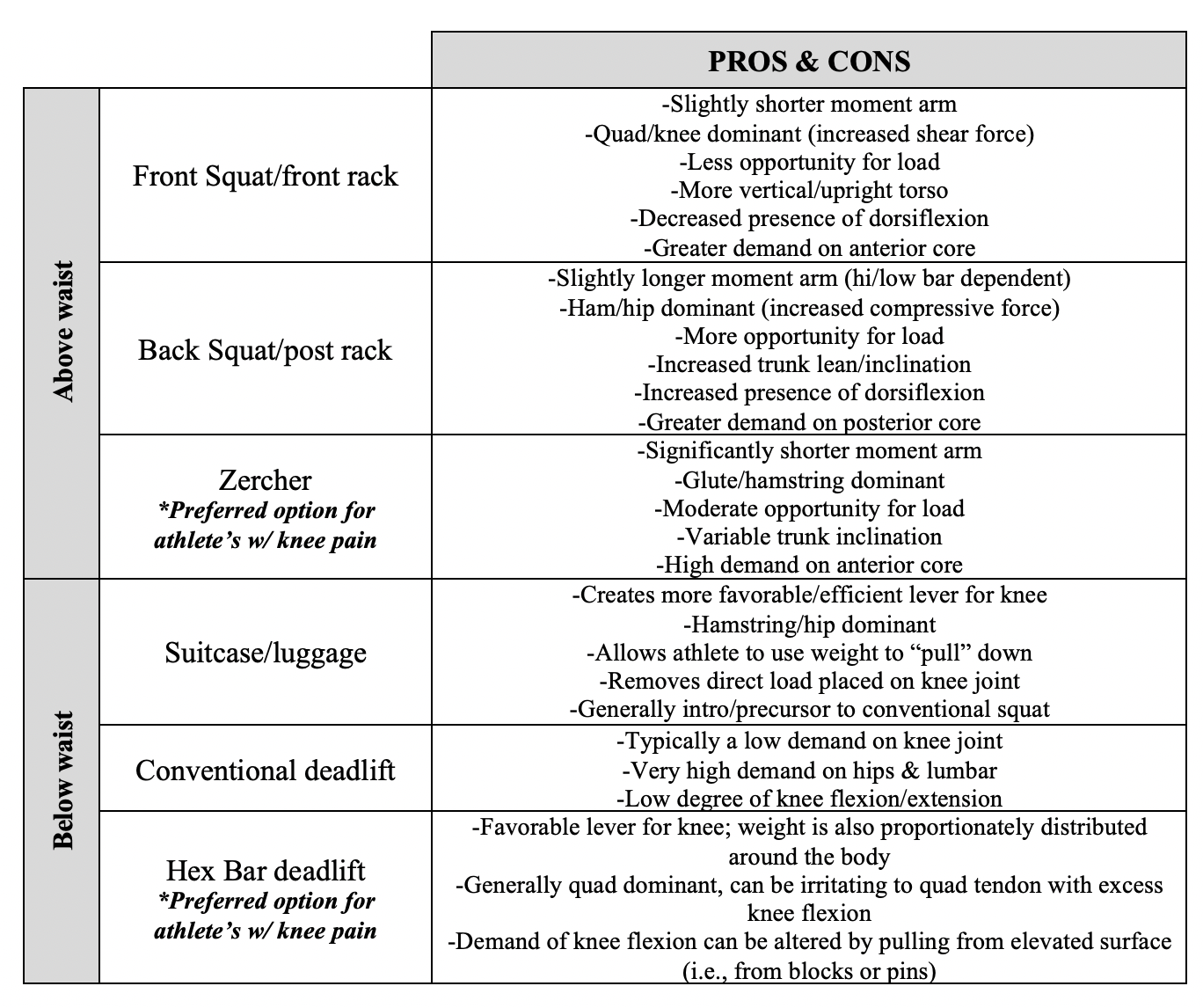
Broadly speaking, having the load above the waist is going to be more demanding on the knees. Mechanically this is because above the waist (i.e., goblet or front rack hold) creates a 3rd class lever, which is relatively inefficient for force production. Conversely, holding below the waist (i.e., suitcase or suspended hold) creates a 1st class lever which is more mechanically efficient. Speaking to the muscles, loading above the waist will largely be more quad dominant and increased stress on the quad tendon. Whereas loading below the waist is more hamstring dominant in nature. The chart below discusses some other common above/below waist loading strategies and their respective pro’s/con’s:
Bringing It All Together
While the knee is a simple joint, it can be a challenging one to work around in the gym. If you’ve had persistent knee pain for several months, my advice would be to have a physician or PT/ATC look at it to make sure there isn’t true injury. For those coming off of a diagnosed injury, and those who just tend to have intermittently bothersome knees, I believe the points outlined above are good principles to follow. My inherent goal working with injured athletes is to reduce the margin for what they perceive to be “not applicable” for them, and what is programmed into their training. The thought should rarely be binary, rather than just omitting or avoiding things entirely, look to see how you can modify the parameters to create a prudent variation for you or your athletes. The goal with restorative training should always, always include re-establishing the confidence of your athletes. In addition, some key technical points:
-Trunk angle is a highly influential squat variable
-->More inclination = shorter moment arm, less demand for quad tendon
-->More vertical = longer moment arm, less demand for hips/lumbar
-Dorsiflexion angle is also vital to consider
-->More DF = less shearing force, but increased compressive force
-->Vertical Shin = more shearing force, reduced compressive force
-Placement of load
-->Above waist = quad demand
-->Below waist = patellar demand
-Don’t ignore fundamental variables (i.e., POM, ROM, speed, volume, intensity)
-Consider blood flow techniques as therapeutic applications
-->Flossing, cupping, blood-flow restriction (BFR) training
-If pain persists beyond a couple of weeks, the training adjustments weren’t correct or technique is not correct
