
Understanding Mechanisms of Injury
As human performance coaches we tend to get absorbed into our own ability to influence or determine outcomes. As I covered in previous articles, injuries are complex, multifactorial events that have very individualistic outcomes. Moreover, although our ability to improve performance has risen dramatically across the last 20 years, sport-related injury trends, if nothing else, remain concerning (1, 2, 6, 9, 14). In other words, we seem to be getting better with improving performance outcomes but have seemingly yet to do the same for mitigating injury risk. And no differently than the debates regarding our ability to influence injuries through training, examining how they occur is an equally confrontational discussion.
Understanding Injury Types
There are two broad classifications of injuries- acute and chronic. We can also organize injuries as being contact or non-contact injuries, with non-contact typically being the more captivating in the performance industry. And the proverbial question with injuries always prevails- can we predict or prevent them?? Well, before we can divulge in that, we need to make a few distinctions. For instance, analyzing the two injuries shown below:


In the top picture, we have one of the most gruesome injuries in NFL history when Alex Smith sustained a spiral, compound lower leg fracture in 2019. On the bottom, another notorious injury from the 2024 super bowl when Dre Greenlaw unfortunately ruptured his Achilles running on the field for the second half. About as contrasting examples you can find to demonstrate the spectrum of injury types or mechanisms.
You’d be hard-pressed to find someone who would say that the Alex Smith leg fracture was in any sense a ‘preventable’ injury, but what about Greenlaw? About as pure of a definition for a non-contact injury mechanism as we will see, and statistically occurring at a very unusual point in the season (see graphic below). We may accept Smith as simply being a devastating and unfortunate situation, but was Greenlaw a situation of “could’ve been prevented”? Where do we determine the line for “unfortunate” and “preventable?”
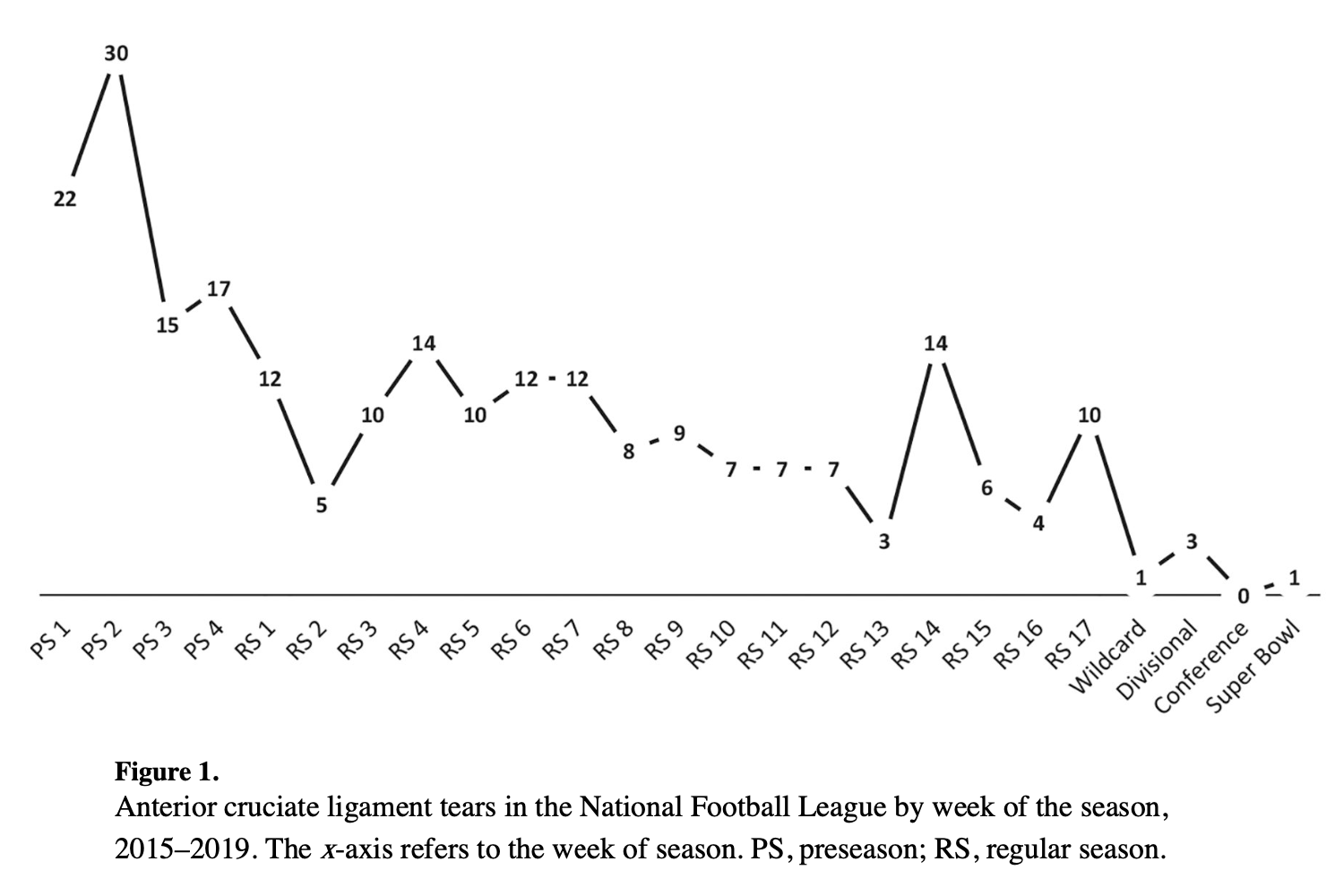
Graphic from Palmieri-Smith, RM (13) showing the number and timing of ACL tears in the NFL. As depicted here, the vast majority of soft tissue injuries occur in the pre-season and early part of the season. This makes the timing of the Greenlaw very perplexing.
Because of the nature of non-contact injuries, particularly like the Greenlaw example, practitioners and researchers have speculated as to whether these injury types should be seen as being preventable (7, 9, 13). In accordance with our increasingly precise ability to track and measure outputs in performance, it’s fair to question what we are missing with perturbing the onset of these types of non-contact injuries.
Individuality of Injuries
No two injuries are the same- not even the same injuries. Due to a wide range of factors and influencing variables, athletes and individuals possess uniquely different interactions with injury. This is why injury mechanism is such a complex conversation and explains why we see so much conflicting information (and opinion). Not only is there incongruence on what specifically causes or contributes to injury, there is also a wildly individualized outcome to injury patterns. For example:
Why does Durant rupture an Achilles on such a rudimentary and routine sequence, but Dennis Smith doesn’t get injured during that landing? Mechanics can defy outcome, and therefore can be deceiving for us to observe and interpret. This also applies for how we consider injury mechanisms for the sake of training prescription and planning. Nevertheless, despite these outlier (“n=1”) cases, there is also a reasonable amount of consistency in areas of injury mechanism we should be aware of.
So, Why Do Injuries Occur?
Soft tissue injuries fundamentally occur when the stress applied to the tissue exceeds its strain capacity. However, importantly, force is not the standalone or even primary factor for many soft tissue injuries. Beyond the force excursions, primary factors for non-contact injuries include body position, foot position, the relationship between those two, the velocity of movement, direction and rate of applied force, and neurocognitive demands of the task. Several soft tissue injuries, particularly non-contact, are a result of tissues being loaded faster than they’re able to respond. And these adjacent factors, beyond the force, all contribute to that outcome.
For instance, analyzing mechanism of injury (MOI) for hamstring strains we can observe the relationship between the stance and swing phases and how this influences the timing of forces applied. As evidenced below, the timing of ground contact (braking phase) predisposes the propulsive phase. Disruption in this timing alters the torque experienced at the hip and knee joints which then directly influences the stress imposed on the hamstrings.
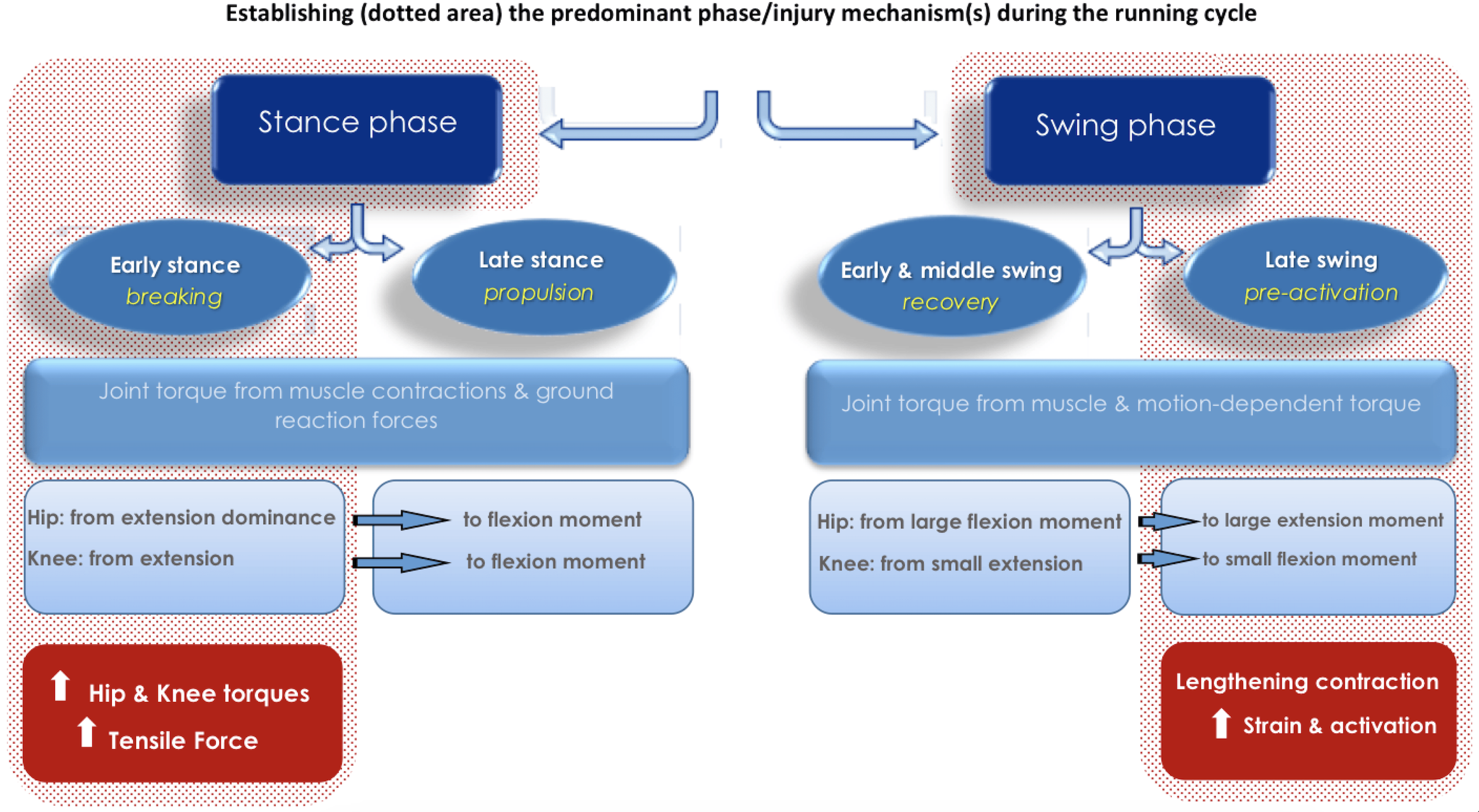
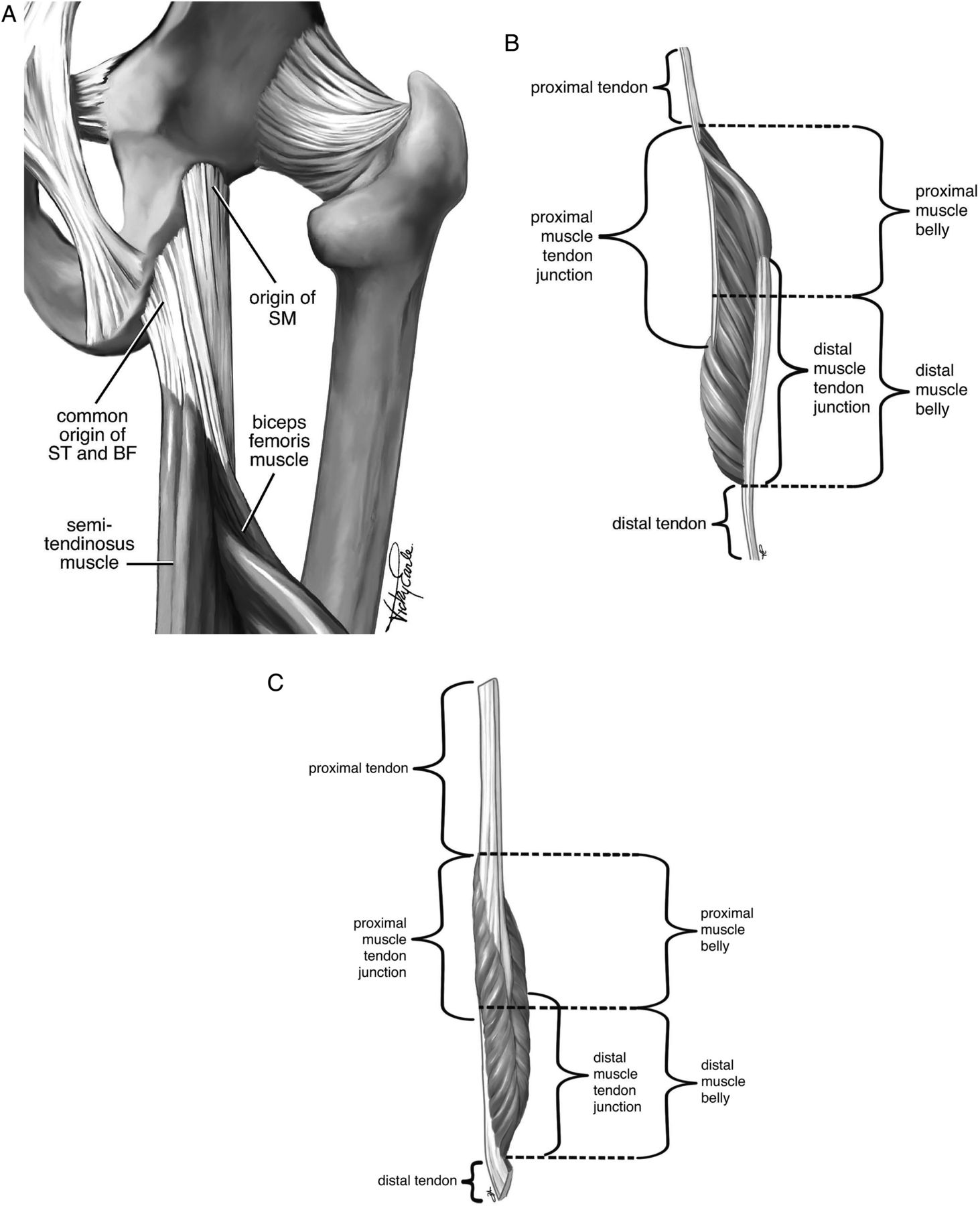
Recall that the hamstrings, namely biceps femoris, are a bi-articulate muscle group that act as both hip extensors and knee flexors. Most hamstring strains occur during late swing phase of sprinting, which occurs as the athlete is approaching touch down- rapidly extending the knee while the hip is flexed (i.e., rapid lengthening followed by rapid shortening from both ends). The rate at which the musculotendinous junction is being stretched, and the pull from both proximal and distal ends results in overstraining of the myofascial and muscle tissue. We should also remain mindful of how trunk position and foot position are also at-play here, regarding hamstring length and actions.
It has also been reliably demonstrated across multiple studies that a significant number of non-contact injuries occur during deceleration and/or cutting actions (4, 5, 11). The aspect of deceleration and change of direction underscores the importance of developing a robust eccentric capacity (i.e., eccentric RFD, braking impulse). However, with deceleration and cutting actions body position and mechanical relationships are also an essential factor.
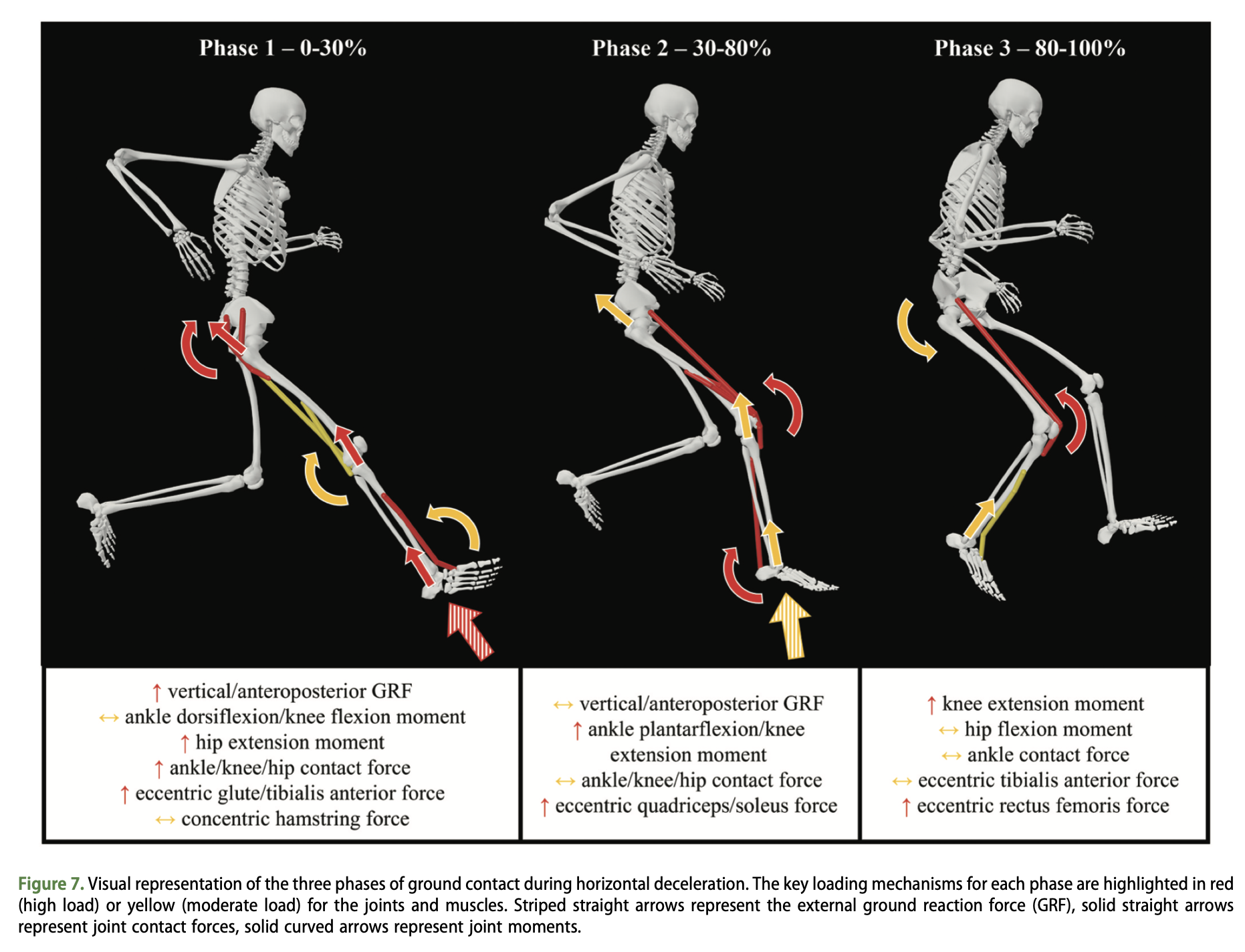
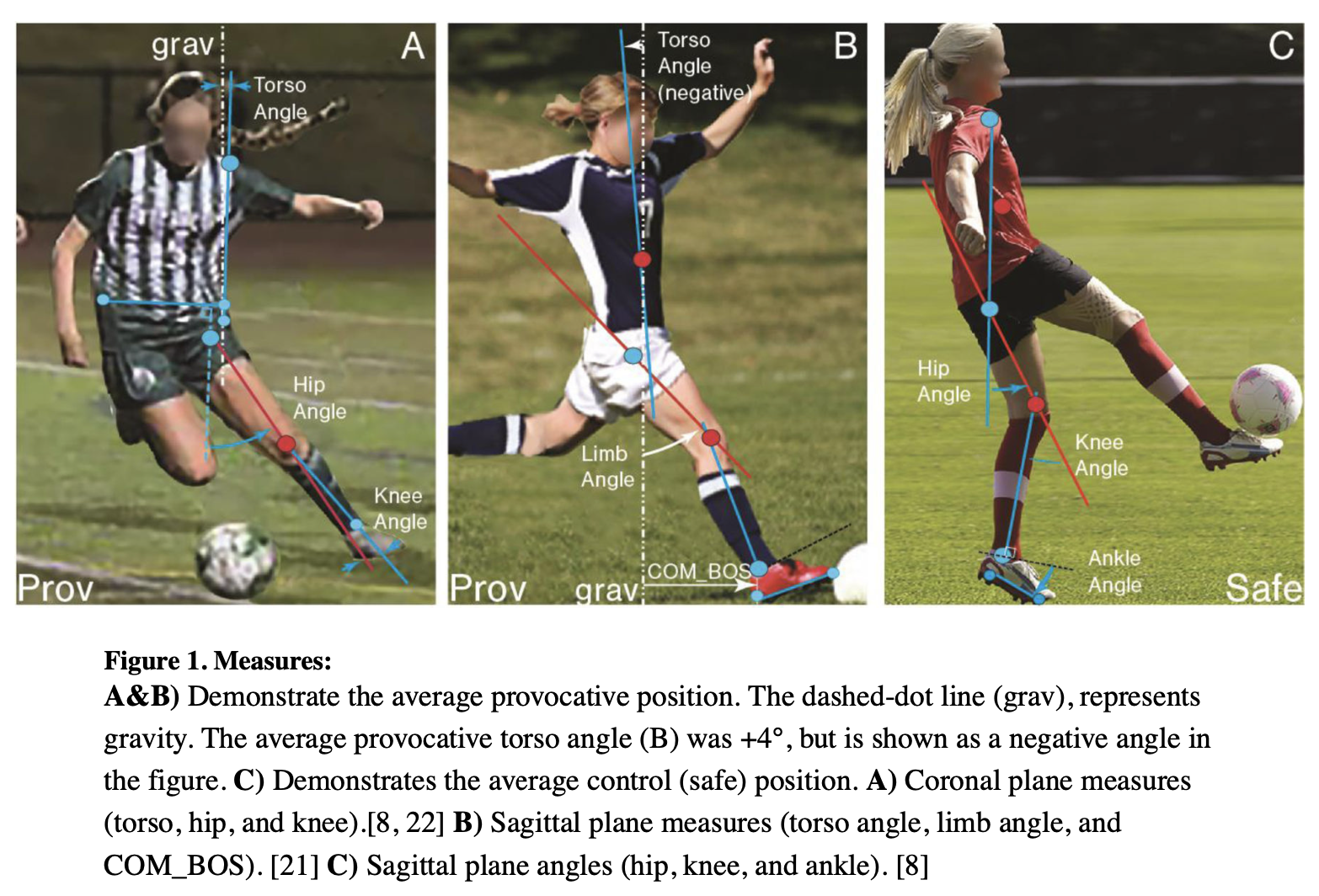
A study from Boden & Sheehan (2) demonstrates this significance as it relates to ACL injuries by showing the relationship between athlete base of support relative to their center of mass (BOS_COM). The further the foot (and center of pressure) is from the center of mass, the greater the torque experienced at the joint/tissue. Training prescriptions should account for the displacement of foot position and seek to improve the athlete’s ability to load and stabilize across a variety of positions/placements.
If we take this and relate back to the videos shown above, the forces only speak mildly to why these injuries occur (i.e., Kevin Durant and Greenlaw). Body position and mechanical relationships are undeniably a factor for non-contact injuries. This is evidenced in both the Greenlaw and Durant, which feature the most conventional MOI for Achilles ruptures- body going forward + leg going back + accelerate with a displaced heel.
Closing
The mechanical factors of injury often get contentious amongst coaches and sport scientists. In my view, we prepare for tasks through familiarization, so for most athletes, I see “an improved ability to tolerate variability” as a defining attribute. While I fully understand the training setting is not meant for sport mimicry or ‘skills training’, I do believe a lot of S&C time can be more diversely (and better) spent. We not only want to expose the athlete to the forces observed in sport, but also the positions, speeds, and situations they’ll encounter as well.
Having a greater bandwidth for movement variability and demand is the underpinning to injury resilience and thus, prevention. Once establishing the proverbial requisite foundation of strength, we want to then challenge the ways in which this strength functions. Almost every sport is a microcosm of chaos, and movement is the expression of a highly complex, dynamic system. Our programming cannot be overtly linear, redundant, and predictive and expect to adequately prepare athletes for demands of sport. Don’t train robotically to play chaotically.
References
1. Allahabadi, S. Gatto, AP. Pandya, NK. 2022. ACL tears in the NFL from 2013-2020. Ortho J Sports Med, 10(2).
2. Bi, AS. Azam, MT. Butler, JJ. Alaia, MJ. Jazrawi, LM. Gonzalez-Lomas, G. Kennedy, JG. 2023. Increased incidence of acute achilles tendon ruptures in the peri-pandemic COVID era with parallels to the 2021-22 NFL season. Knee Surgery, 31:2160-2165.
- Bittencourt, NN. Meeuwisse, WH. Mendonça, LD. Nettel-Aguirre, A. Ocarino, JM. Fonseca, ST. 2016. Complex Systems Approach for Sports Injuries: Moving from Risk Factor Identification to Injury Pattern Recognition—Narrative Review and New Concept. Br. J. Sports Med, 50, 1309–1314.
- Brophy, RH. Wojtys, EM. Mack, CD. Hawaldar, K. Herzog, MM. Owens, BD. 2021. Factors associated with the mechanism of ACL tears in the NFL. Ortho J Sports Med, 9(11).
- Boden, BP. Sheehan, FT. 2022. Mechanism of non-contact ACL injury: OREF clinical research award 2021. J Orthop Res, 40:531-540.
- Ekstrand, J. Bengtsson, H. Waldén, M. 2023. Hamstring injury rates have increased during recent seasons and now constitute 24% of all injuries in men’s professional football: the UEFA Elite Club Injury Study from 2001/02 to 2021/22. British Journal of Sports Medicine, 57:292-298.
- Gabbett, TJ. 2016. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med, 0:1-9.
- Hewett, TE. Lavender, CD. Schaver, AL. 2024. An Apparent Achilles Heel of the NFL: Have Achilles Tendon Injuries Significantly Increased to Unacceptably High Incidence Levels in the NFL and if so, why? A Clinical Insight. IJSPT,19(2):145-147.
- Huang, YL. Jung, J. Mulligan, CS. Norcross, MF. 2020. A Majority of Anterior Cruciate Ligament Injuries Can Be Prevented by Injury Prevention Programs: A Systematic Review of Randomized Controlled Trials and Cluster-Randomized Controlled Trials with Meta-Analysis. Am. J. Sports Med, 48, 1505–1515.
- Hulme, A. Thompson, J. Nielsen, RO. Read, GM. Salmon, PM. 2019. Towards a Complex Systems Approach in Sports Injury Research: Simulating Running-Related Injury Development with Agent-Based Modelling. Br. J. Sports Med, 53, 560–569.
- Huygaerts, S. Cos, F. Cohen, DD. Calleja-Gonzalez, J. Guitart, M. 2020. Mechanisms of hamstring strain injury: interactions between fatigue, muscle activation, and function. Sports. 8,65.
- Lawrence, DW. Comper, P. Hutchinson, MG. 2016. Influence of extrinsic risk factors on NFL injury rates. Ortho J Sports Med, 4(3).
13. Liveris, NI. Papageorgiou, G. Tsepis, E. Fousekis, K. Tsarbou, C. Xergia, SA. 2023. Towards the Development of a System Dynamics Model for the Prediction of Lower Extremity Injuries. Int. J. Exerc. Sci, 16, 1052–1065.
- Palmieri-Smith, RM. Mack, CD. Brophy, RH. Owens, BD. Herzog, MM. Beynnon, BD. Spindler, KP. Wojtys, EM. 2021. Epidemiology of ACL tears in the NFL. Am J Sports Med, 49(7)1786-1793.
15. Verheul, J. Harper, D. Robinson, MA. 2024. Forces experienced at different levels of the musculoskeletal system during horizontal decelerations. J Sports Sciences, 42:23, 2242-2253.
