Assessing & Evaluating Athletes
As with almost anything in strength and performance training, there isn’t a right or wrong way to go about evaluating your athletes (within obvious reason). Everyone has their own approach, and there can be a valid advocation for a litany of these approaches. Formalized assessments have been around for decades, but have been subject to criticism more recently, and for somewhat justifiable reason in my opinion. It was particularly rampant following the explosion of the Functional Movement Systems (FMS) developed roughly a decade ago by renowned physical therapists Gray Cook and Lee Burton. The FMS essentially popularized assessing athletes/clients by introducing a comprehensive, uniformed system that produced tangible ‘grades’ and classifications. This system was excellent in theory but had its shortcomings practically. We’ll discuss more on this in a bit though.
Where the FMS is developed around an athlete’s ability to demonstrate proficiency in global ‘functional-based’ movements such as the overhead squat and inline split squat there are other approaches to assessing athletes such as the Neurokinetic Therapy (NKT) method. NKT, developed by David Weinstock, describes itself as a “connective movement system that addresses the cause of pain”. The NKT method, which is objectively somewhat more complex than something like the FMS, is based on muscular activations and their relationships to other muscles; namely the functional opposites or antagonist muscles. In theory, every muscle has an optimal firing ability (or contractility) and optimal recruitment in regard to firing sequence. Meaning, we can independently test muscular activation, then subsequently test other muscles to see if each is firing and if it’s firing correctly. It should go without saying, there is a long line of critics for these types of assessments or even just beliefs in general. But that’s not the focus of this article.
Point being, these are just two of hundreds of formalized assessment certifications. They also happen to be the two that I hold as well. Personally, I think both FMS and NKT have merit, obviously considering I invested in them. But I don’t disagree with some of the knocks and opposing viewpoints. As with damn near everything, I feel like there is good logic behind FMS and NKT and others, but it’s incumbent on the coach to integrate them into their practice with autonomy and good judgement. I use the NKT principles in my assessment, but it isn’t the start and stop point. I use the active straight leg raise (FMS item) in my assessment, but I don’t understand a point in giving the athlete a “score” for something that’s going to improve because we’re gonna work on it. The most important things above anything else are A.) you have an actual dedicated assessment, B.) your assessment makes sense to YOU and C.) you actually address the things you point out in your eval and reference the notes you took on them. If those items are met, the world is yours and we’re just living in it.
I.) Know what you’re looking for
It’s always at the forefront of our conversations but can’t be emphasized enough- you MUST know your anatomy. Wouldn’t make much sense to have a mechanic look at your car if they don’t know what a transmission looks like, right? But in all seriousness, this is where knowing your specific muscle actions comes into play. Let’s take the rotator cuff muscles as an example. Lets say you detect dysfunctions in overhead flexion, instead of just jotting down “OH flexion is off” and/or simply avoiding overhead movements altogether, you now have the ability to make programs/training sessions highly specific and effective. In this hypothetical, let’s say you identified the athlete wasn't able to fully externally rotate their hand as they went overhead. This allows you to assume their restriction is likely due to a weak infraspinatus (external rotator) or tight subscapularis (internal rotator) because they weren’t able to externally rotate the arm very well when going into flexion. Now, you can program more specific and effective exercises down the road, as opposed to just avoiding the area or misapplying exercises.
That feeds right into the next point, which is never test “just to test”. It does you no good to waste time on something you either don’t understand or aren’t going to address. I know there’s always pressure to demonstrate to the athlete that you know what you’re doing, but it’s just as important to remember scope of practice and knowledge boundary during assessments as it is during training. I’ve always treated assessing my athletes as if I were in an anatomy lab, it’s a critical opportunity to learn your athlete, but it’s equally a tremendous opportunity to challenge your level of thinking/ability and learn. Anytime something looks off, or the athlete comes in with something you’ve yet to work with, it should spark an excitement to do your homework and dig deeper on things you’re not yet familiar with. Don’t be intimidated by things you see or come across; embrace the challenge of learning something new and ultimately expand your toolbox for athletes to come down the road.
Another thing I like to be cognizant of is knowing your specific population as thoroughly as you can. It will give you a better starting ground for assessing them biomechanically, and a narrower window for where you should invest your time/attention. For instance, I now work exclusively with a military population. There is an extremely high degree of overlap between my athletes. Not only do they all have the same background in terms of work/duties, but the majority have very similar body types, postures and even injury histories. Taking the time to understand what their day-to-day looks like and how their duties are performed can significantly improve your ability to assess them. Frankly I didn’t know shit about the ins and outs of the military world and what they were subjected to when I first started working with this population. But I did everything I could to learn more about them as quickly as I could. A few things I did early on were going and doing some of the things they’re frequently tasked with, such as going and doing an O-course myself, understanding their equipment, and asking direct questions about training, deployments, etc. I also started watching a ton of YouTube videos on skydiving, fast roping, and combat action. Needless to say, it’s given me a much better perspective of where these men and women are coming from which has vastly improved my ability to assess and work with them.
II.) Global-Static
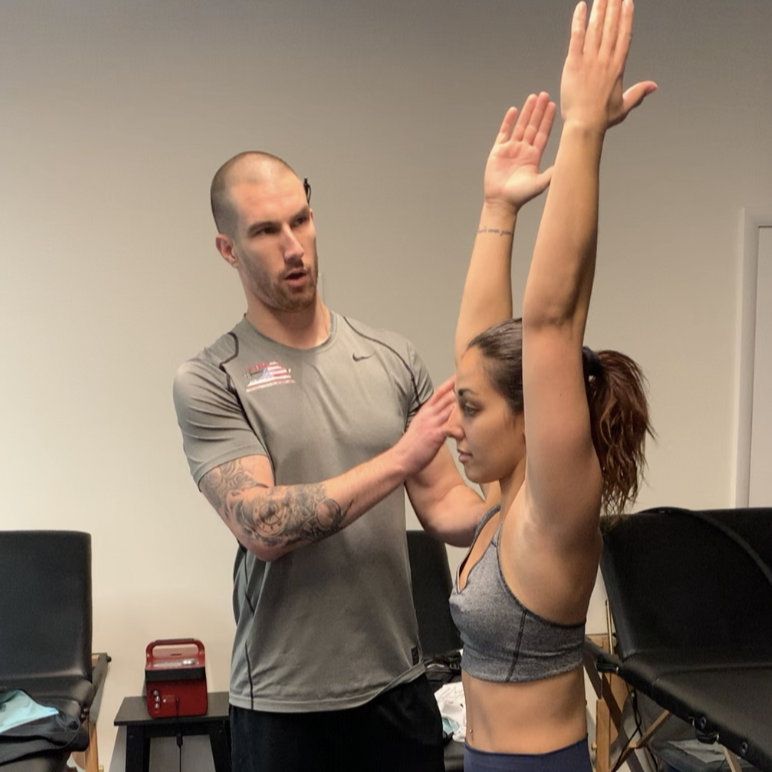
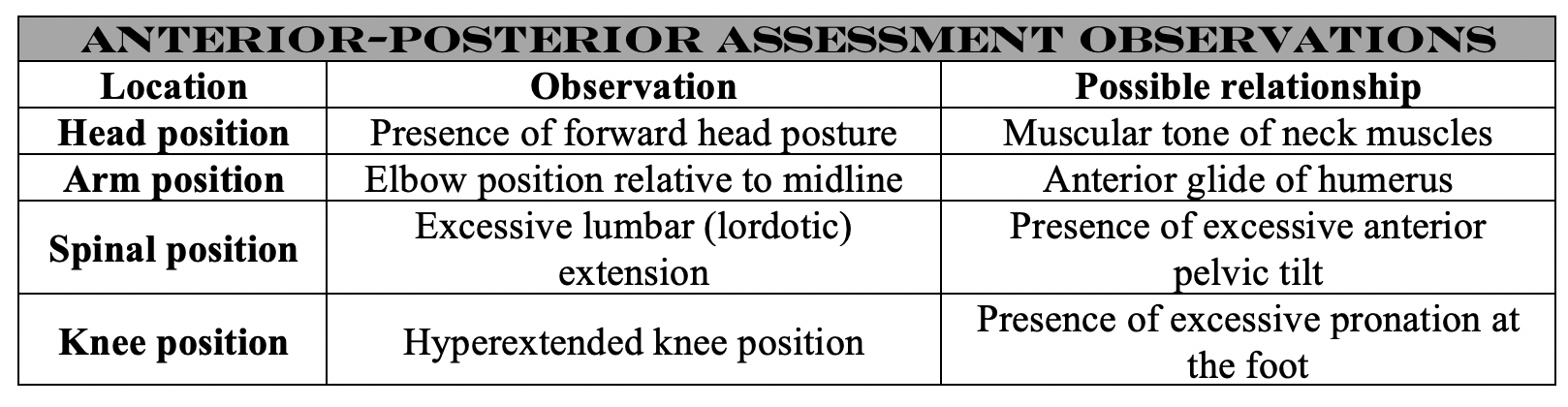
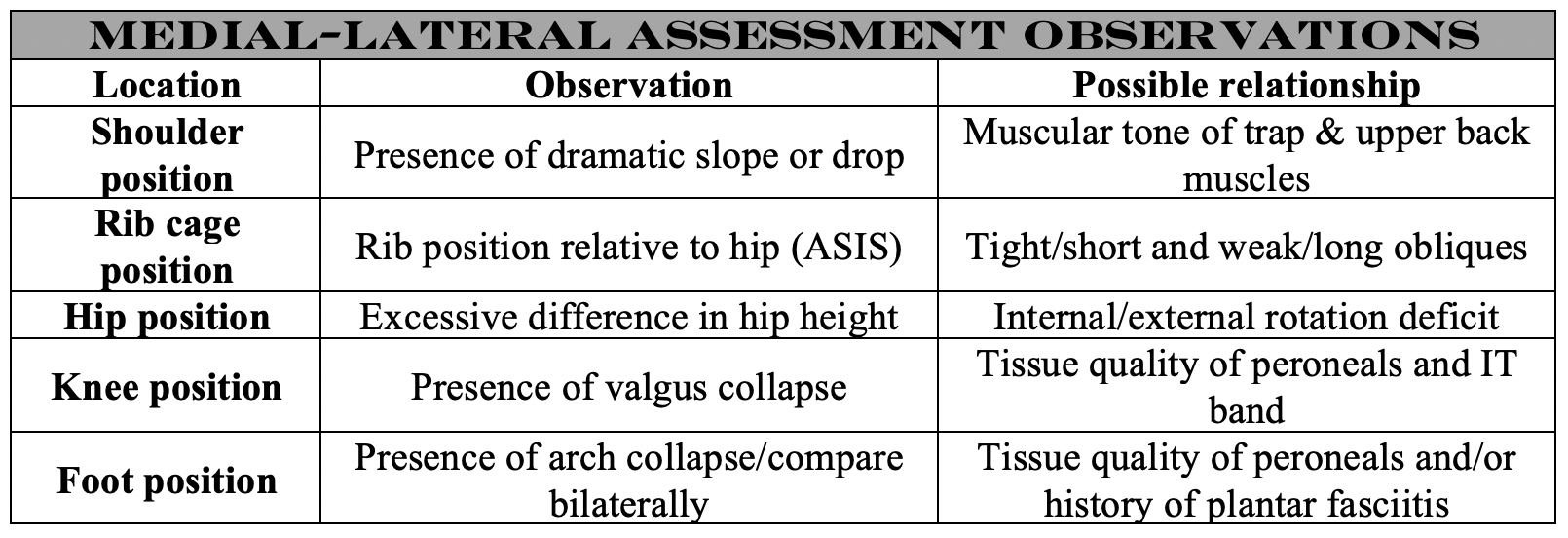
Everything in the assessment starts with a static, total 360° view of the athlete. I do feel it’s important to have them out of their shoes and remove their shirt (if context/situationally appropriate). Clothes can mask a lot of important postural observations; thus, I feel it’s necessary to see as much directly as possible. When I’m doing a global observation, I first want to look for a general “feel” of their resting posture. Do they look tense or guarded? Are they favoring one side or the other? Do they feel uncomfortable being analyzed or having their shirt off? Does it look like they’re masking something? In addition, these are the more biomechanical items I’m looking for:




III.) Global-Dynamic
Once we’ve observed our athlete statically, it’s time to put them in motion. It’s important to treat static and dynamic assessments somewhat differently. In a static situation, the athlete has the advantage to put themselves in certain positions and in essence coverup potential dysfunctional areas or areas of weakness. Furthermore, not only are you putting them in specific positions during a static assessment, but you can also hold them there for as long as needed. This is why I feel it’s important to film your dynamic evaluations. There’s always a lot going on, and you only have so much time to put someone through tests and assessments. So I normally record every athlete I work with, and make sure I watch the film that night at home to collect more detailed notes. The easy analogy here is thinking about the car with loose lug nuts. If we take that car slowly around the block at 20 mph, we may not think there’s anything wrong. We take that car out on the interstate at 60 mph and shit’s gonna start to expose itself. Here’s an overview of some of my main criteria for a global-dynamic assessment:
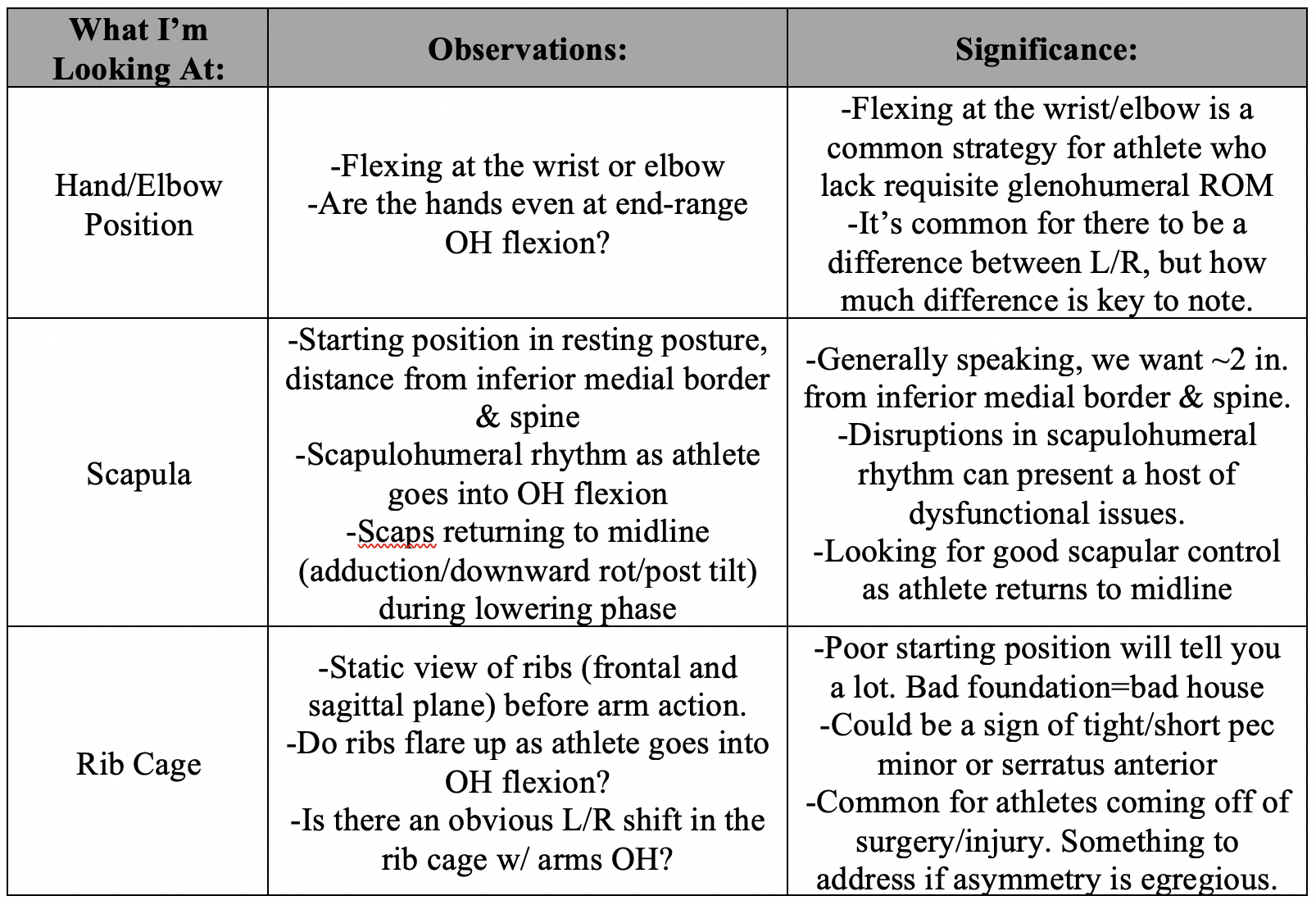
OH Flexion:
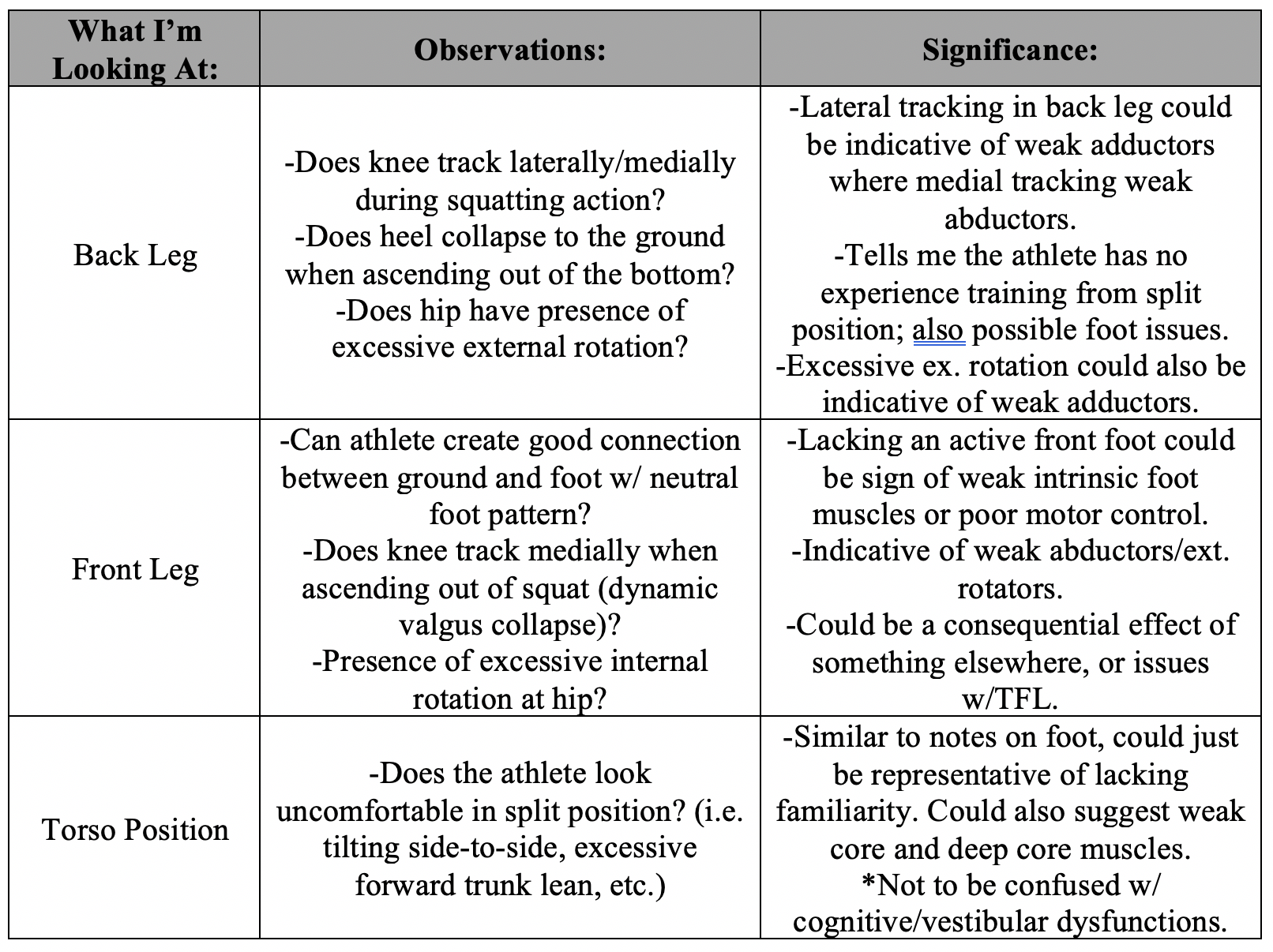
Split Squat:
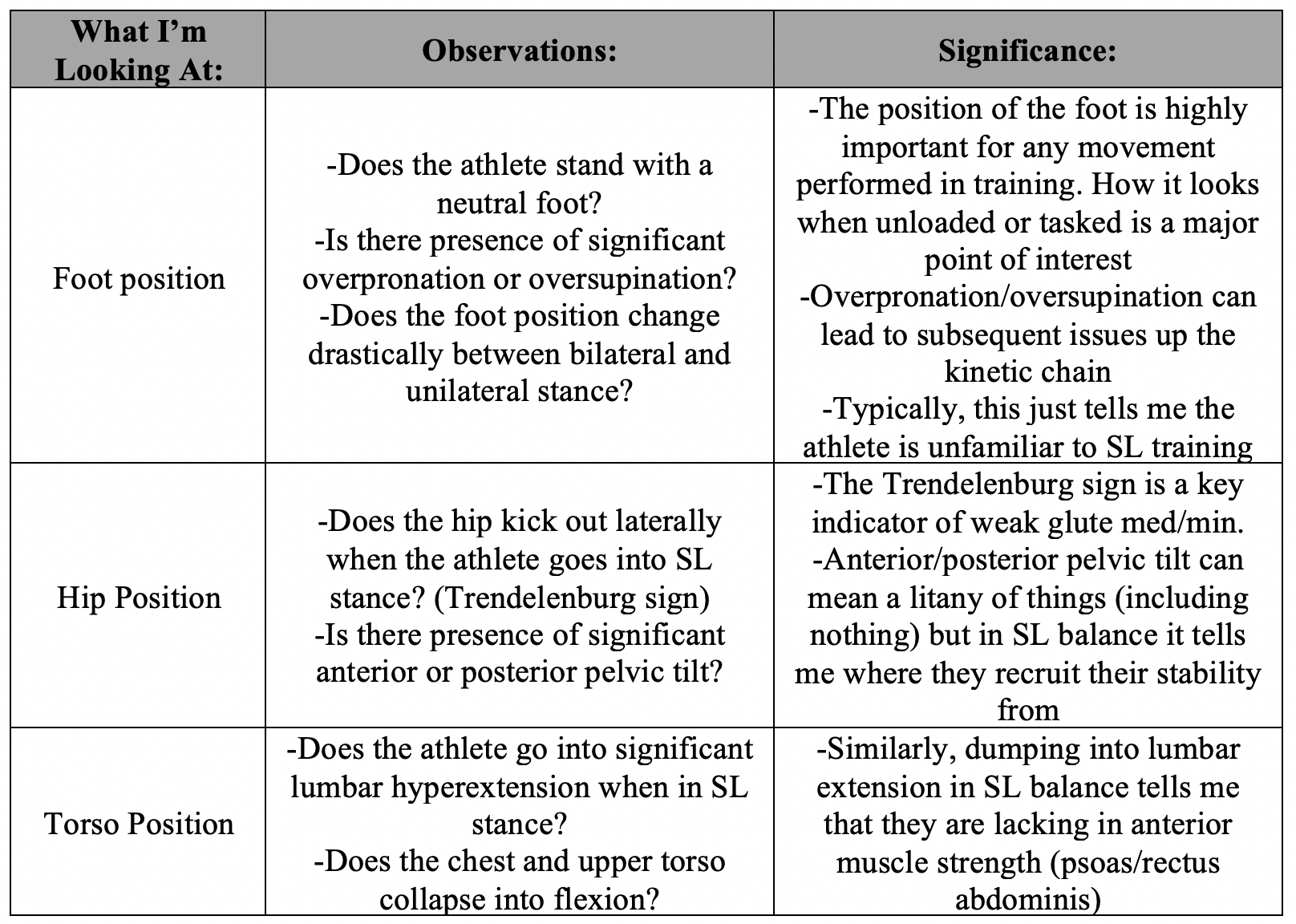
Single Leg Balance:
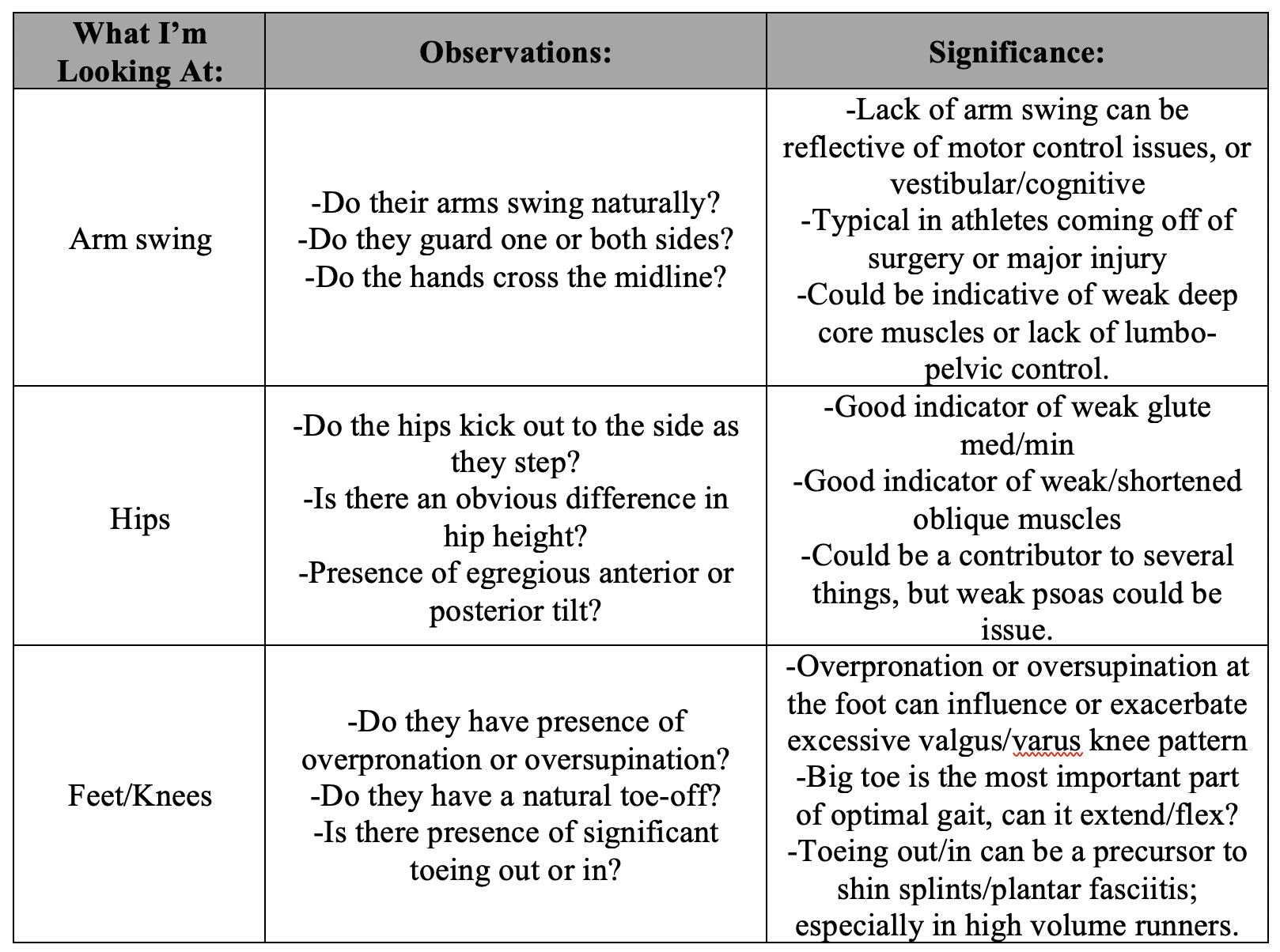
Very informative video via Yoga Anatomy Here: Gait Analysis
IV.) Manual Muscle Testing
I suppose I have to start this section out by reiterating scope of practice. In our field, everything changes in a major way when we put people on tables and start putting our hands on people. I’ve been very fortunate throughout my career thus far to not have any incidents with regard to scope of practice or injuring someone. But man, I’ve heard some really wild and unfortunate stories from people, so it’s always something that needs to be at the forefront of your mind. I’m very lucky that my place of work has a high-quality camera system throughout the gym. I rely heavily on this. Especially when I’m doing my assessments or making direct physical contact with my athletes at all, I am always sure to be directly under a camera- just in case. In any event, use good discretion, and don’t ever violate your scope.
Manual muscle testing is a way that we can isolate a particular muscle to check and see if it’s firing properly. Additionally, we can then check individual muscles and see how they relate to other muscles or compare bilaterally to the same muscle. As far as I’m concerned, manual muscle testing is really just giving me a better idea of muscular relationships:
-How does the psoas relate to the ipsilateral glute and contralateral psoas?
-How does the hamstring relate to the ipsilateral glute and contralateral QL?
-How does the lat relate to the ipsilateral serratus and contralateral trap?
The caveat to this is that they could mean everything, or they could mean nothing at all. Again, I can’t stress this enough, we’re not looking to see what’s “broken” or deliberately trying to find every little muscle that can be deemed “dysfunctional”. All we are looking for is how this individuals’ muscles fire, how they compare bilaterally, and then how they relate to other muscles thereafter. It’s also important to recognize that we are NEVER looking to diagnose anything. Not only is that far from the responsibility of a strength coach, but without a comprehensive protocol (including imaging) we literally can’t diagnose anything. Once again, this is just us mapping out what we’re working with and using what we find in our assessments to strategize and plan our approach.
I think of this like putting together a puzzle. Using whatever theoretical values or systems you confide in, there is an optimal length/tension relationship and optimal contractility for every muscle in the human body. When we conduct these assessments, we want to see how the athlete compares to theoretical norms and determine whether or not we feel this athlete has areas of clear weakness or concern for whatever their performance demands of them. Everyone has strengths and everyone has weaknesses, and this is something that is highly individualistic. This is where the whole puzzle metaphor comes into play- what are the athlete’s strengths, what are their weaknesses, what’s the pecking order of what we need to address in the time we have? I'm not going to include videos for this, but using whatever technique or protocol you prefer, I typically always test the following:
-Lat, serratus, upper/lower trap, and rhomboids
-Hamstrings, glutes, psoas, adductors and quads
As I mentioned above, we should have a good understanding of the populations we work with. Using my own population as the example here, I know that roughly 3/5 athletes I see will have either a SLAP or rotator cuff injury or surgical history. Additionally, I know that roughly ¾ will cite low back pain as a major inhibitor and/or have history of major spinal surgery. So, in addition to the common sites outlined above, I will also almost always conduct localized testing on the shoulders, neck, and lumbopelvic region. Again, for the sake of professional scope, I'm not going to include videos here, but there are countless YouTube accounts you can search for these.
The last item I want to look for with manual muscle testing is the anterior and posterior fascia slings. The function of the anterior and posterior fascia slings are critical for optimal performance and eradicating non-descriptive chronic pain. In short, if we have disruption with either the anterior or posterior sling, it can result in muscles becoming underdeveloped or hyperactive. This can lead to disruption in muscular firing patterns, whereby prime movers become synergists, synergists become prime movers, or muscles shut down entirely.
Anterior Sling: Combination of obliques/pec minor + contralateral adductor
Posterior Sling: Combination of lat + contralateral glute
Lateral Sling: Effectively the obliques and ipsilateral lat
V.) Isolated- Passive/Assisted
Every athlete I work with will be evaluated on the criteria outlined up to this point. From the global-static assessment all the way through to manually testing the fascial slings, I will take every single athlete through those steps. Once we get to isolated-passive/assisted assessments, this is not something I will do for everyone. I reserve this and the following phases of assessments only for those who warrant it. For example, if I have an athlete coming off a rotator cuff tear, I will take these subsequent measures to assess the shoulder with more detail. The reason I don’t take everyone through these more refined assessments relates back to two things:
1.) I’m not a doctor. Therefore, my job or goal isn’t to diagnose. If they haven’t had something clinically documented, it doesn’t make sense for me to assess it because I could create a false positive or false negative. (Some exception for those who may not have something formally diagnosed but has a chief complaint on a specific area).
2.) Time. I only have a limited window to take someone through an assessment. It can become counterproductive quickly to take someone through a bunch of tests they likely don’t need. I don’t have any interest in wasting my time or the athletes… get them through the base level assessment and if something further is required, do it. If not, move on.
But, in the event someone does require additional testing, it would be equally imprudent to just skip over it. Most of what I do for isolated-passive/assisted assessments comes directly from the conventional testing we were all introduced to in our academia and the special testing items shown above.
VI.) Isolated- Active/Resisted
The final step would be to take the athlete though active or resisted manual testing. This is essentially the same exact tests outlined above, only performed actively or against modest resistance. Once we clear them taking them through a manual test passively, we can then take them through the same pattern but either have them perform on their own or even against light manual resistance. One thing I will also include in this stage though is looking at the difference in active and passive ROM at certain areas. Hip internal and external rotation is one of my most common areas of interest for this. I’ll take the athlete through the ROM passively, then have them go through the same ROM actively and assess the difference between the two. (Be sure to wait like 30 seconds between movements, you moving them passively will ‘loosen’ the area transiently). But what this could likely mean is that the athlete has too much difference between active and passive ROM. Consequently, this could be a variable in injury manifestation because the joint can move in certain degrees of motion but cannot actively control it.
VII.) Bringing it All Together
Just to recap the big criteria when we’re assessing our athletes, here are my major points:
-You’re not a doctor, you’re not a physical therapist. We are strength/performance coaches. Scope of practice is critically important.
-We are NOT looking to diagnose. We are simply collecting information and observations the athlete presents.
-Have the athlete out of their shoes, and ideally out of their shirt.
**Always be transparent with your athletes. If you’re going to have them remove clothing, or make physical contact, ask them if they are comfortable with it first. If you’re going to film them, get their consent first and be sure to reiterate that this will not be shared publicly.
-Know who you’re working with/what you’re looking for. NEVER test just “to test” and never tell the athlete information that you aren’t qualified to discuss.
-Once we gather our information, it is extremely important to sit down and review the notes. Do homework on things that don’t make complete sense to you and put together a plan of action for training.
-If you took specific measurements or have tangible criteria in your assessment, be very sure that these items will be directly addressed in training. It makes no sense to measure things only to avoid them, follow through on what you’re assessing.
-Use this opportunity to build an archive for your private files. I refer back to athletes I’ve worked with often and used them as learning points. You will almost always see athletes later on that present similar postures/dysfunctions/movements. The more you see, the more you should be referencing back.
